Você também pode gostar
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- SplintingDocumento4 páginasSplintingMayer Rosenberg100% (1)
- Examination of The HandDocumento20 páginasExamination of The HandOtnil DAinda não há avaliações
- Effects of Scapular Stabilization Exercise Training OnDocumento12 páginasEffects of Scapular Stabilization Exercise Training OnNajoua SalomaoAinda não há avaliações
- Netball Rubric F1Documento2 páginasNetball Rubric F1Ronald AliAinda não há avaliações
- Bones of the Forearm: Radius and Ulna AnatomyDocumento1 páginaBones of the Forearm: Radius and Ulna AnatomyMihaelaAinda não há avaliações
- Brachial Plexus Outcome Measure (BPOM)Documento1 páginaBrachial Plexus Outcome Measure (BPOM)jesscavalcanteAinda não há avaliações
- Back, Chest, Leg & Shoulder Workout GuideDocumento16 páginasBack, Chest, Leg & Shoulder Workout Guidesambelov100% (2)
- Colles Fracture - PhysiopediaDocumento4 páginasColles Fracture - Physiopediamuhammad iqbal mahfuzhAinda não há avaliações
- Shoulder Impingement RehabilitationDocumento3 páginasShoulder Impingement RehabilitationHamzh Sallam100% (2)
- Peter Duffie - ApplicationsDocumento59 páginasPeter Duffie - Applicationsbobbobov1Ainda não há avaliações
- Muscles of Superior ExtremityDocumento11 páginasMuscles of Superior Extremity[93]-Amrita PramanikAinda não há avaliações
- Upper Trapezius MuscleDocumento6 páginasUpper Trapezius MusclejpAinda não há avaliações
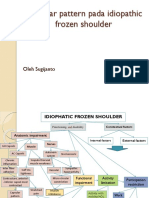
- Capsular pattern identification in idiopathic frozen shoulderDocumento11 páginasCapsular pattern identification in idiopathic frozen shoulderRhany JulyatiAinda não há avaliações
- Pectoral Region & BreastDocumento52 páginasPectoral Region & BreastemanAinda não há avaliações
- Ret Dem or PRSDocumento4 páginasRet Dem or PRSMarimiel PagulayanAinda não há avaliações
- Fraktur Clavicula DextraDocumento28 páginasFraktur Clavicula DextraRaisah_Ridwan382Ainda não há avaliações
- Radius (Bone)Documento8 páginasRadius (Bone)ranshAinda não há avaliações
- Translated Russian To English (Topography Anatomy)Documento110 páginasTranslated Russian To English (Topography Anatomy)Harjun SinghAinda não há avaliações
- Functional Rehabilitation: Mat Techniques: Rolling: Training StrategiesDocumento3 páginasFunctional Rehabilitation: Mat Techniques: Rolling: Training StrategiesDuppala Sateesh KumarAinda não há avaliações
- 4 WHO Standard Acupuncture Point Locations in The Westernpart 4Documento30 páginas4 WHO Standard Acupuncture Point Locations in The Westernpart 4Virgil Anma100% (1)
- Lesões de Punho e MãoDocumento86 páginasLesões de Punho e MãoRobsom InacioAinda não há avaliações
- Brachial Plexus InjuryDocumento8 páginasBrachial Plexus InjurylewienAinda não há avaliações
- 12 Acup Pts Save LifeDocumento7 páginas12 Acup Pts Save LifefreimannAinda não há avaliações
- Ligaments of the Wrist Studied in Dissection of 17 SpecimensDocumento9 páginasLigaments of the Wrist Studied in Dissection of 17 SpecimensEnrique Maturana SepulvedaAinda não há avaliações
- Anatomy 1.4 Upper Limbs - Muscle and FasciaDocumento10 páginasAnatomy 1.4 Upper Limbs - Muscle and Fascialovelots1234Ainda não há avaliações
- Shoulder Joint BiomechanicsDocumento129 páginasShoulder Joint BiomechanicsKhan SalimAinda não há avaliações
- Distal Phalanx (45%) - Metacarpal (30%) - Proximal Phalanx (15%) - Middle Phalanx (10%)Documento40 páginasDistal Phalanx (45%) - Metacarpal (30%) - Proximal Phalanx (15%) - Middle Phalanx (10%)Dabessa MosissaAinda não há avaliações
- 1) Vertebrobasilar Artery InsufficiencyDocumento22 páginas1) Vertebrobasilar Artery Insufficiencybjpalmer100% (6)
- Muscle Stretching in Manual Therapy I - The Extremities (Team Nanban) (TPB)Documento177 páginasMuscle Stretching in Manual Therapy I - The Extremities (Team Nanban) (TPB)CNPOULIS100% (22)
- Chapter 23: The ElbowDocumento48 páginasChapter 23: The ElbowFloriza de Leon100% (1)