Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- GP Letter Example PV-ESRDocumento6 páginasGP Letter Example PV-ESRRyan ChenAinda não há avaliações
- RMR Nr-1 2008 Art-08 RomanaDocumento3 páginasRMR Nr-1 2008 Art-08 RomanaRyan ChenAinda não há avaliações
- Compositional Properties of BloodDocumento10 páginasCompositional Properties of BloodRyan ChenAinda não há avaliações
- Glanders: C H A P T E R 2 - 5 - 1 1Documento10 páginasGlanders: C H A P T E R 2 - 5 - 1 1Ryan ChenAinda não há avaliações
- GlandersDocumento7 páginasGlandersRyan ChenAinda não há avaliações
- Nr. Ord. Țara: Cazuri Focare Cazuri Focare Cazuri Focare Cazuri Focare Cazuri FocareDocumento4 páginasNr. Ord. Țara: Cazuri Focare Cazuri Focare Cazuri Focare Cazuri Focare Cazuri FocareRyan ChenAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Comparative Evaluation of The Nutritional Quality of Corn, Sorghum and Millet Ogi Prepared by A Modified Traditional TechniqueDocumento6 páginasComparative Evaluation of The Nutritional Quality of Corn, Sorghum and Millet Ogi Prepared by A Modified Traditional TechniqueFaldy LeimenaAinda não há avaliações
- Effect of Seed Priming On Seed Quality of Maize (Zea Mays L.)Documento2 páginasEffect of Seed Priming On Seed Quality of Maize (Zea Mays L.)Angela KnightAinda não há avaliações
- Naipunnya Institute of Management and Information Technology, PongamDocumento53 páginasNaipunnya Institute of Management and Information Technology, PongamAlex John MadavanaAinda não há avaliações
- Postharvest Handling and Storage of Fresh Cassava Root and Products A ReviewDocumento20 páginasPostharvest Handling and Storage of Fresh Cassava Root and Products A ReviewMaharani Hazar100% (1)
- More About RiceDocumento10 páginasMore About RiceismvohraAinda não há avaliações
- MOAD Statistical InformationDocumento222 páginasMOAD Statistical InformationSuraj_SubediAinda não há avaliações
- SUNRAY Review of Nutrition Research in AfricaDocumento33 páginasSUNRAY Review of Nutrition Research in AfricaAntoine Nabil ZakiAinda não há avaliações
- BenthamDocumento52 páginasBenthamram100% (1)
- SOLAS CHAPTER 6 Group 4Documento16 páginasSOLAS CHAPTER 6 Group 4Derla JunnielAinda não há avaliações
- General Agriculture 2020 For JRF, SRF Other ExamsDocumento60 páginasGeneral Agriculture 2020 For JRF, SRF Other ExamsTamilarasiAinda não há avaliações
- Budget Diet PlanDocumento3 páginasBudget Diet PlanAngie WandyAinda não há avaliações
- tmp46D7 TMPDocumento12 páginastmp46D7 TMPFrontiersAinda não há avaliações
- Current Status of Food Processing IndustryDocumento19 páginasCurrent Status of Food Processing IndustryAmit Kumar90% (21)
- Lopes, 2023 MycotoxinesDocumento15 páginasLopes, 2023 MycotoxinesRAFIQAinda não há avaliações
- IDirect RallisIndia ICDocumento35 páginasIDirect RallisIndia ICArun DubeyAinda não há avaliações
- A History of Beer and Brewing 2004 - Hornsey PDFDocumento762 páginasA History of Beer and Brewing 2004 - Hornsey PDFjhockstrapp100% (2)
- Lal Qilla Basmati RiceDocumento5 páginasLal Qilla Basmati Ricemittalsakshi020692Ainda não há avaliações
- Science Bulletin: Qijin He, Guangsheng Zhou, Xiaomin Lü, Mengzi ZhouDocumento8 páginasScience Bulletin: Qijin He, Guangsheng Zhou, Xiaomin Lü, Mengzi Zhousunitha dAinda não há avaliações
- Grains and Its Starch ContentDocumento2 páginasGrains and Its Starch ContentkrishnaAinda não há avaliações
- PHE 9th Grade Lesson NOTEDocumento12 páginasPHE 9th Grade Lesson NOTENnia ManiAinda não há avaliações
- Ethiopian Agricultural Investment PotentialDocumento22 páginasEthiopian Agricultural Investment PotentialA.Nafi YürekliAinda não há avaliações
- IFS Trend Risk Report January 2021Documento11 páginasIFS Trend Risk Report January 2021RocioAinda não há avaliações
- A Study On Growth and Performance of Dairy Sector in NepalDocumento13 páginasA Study On Growth and Performance of Dairy Sector in NepalIJEAB JournalAinda não há avaliações
- Book Weed ManagementDocumento15 páginasBook Weed Managementerasmolemus6020Ainda não há avaliações
- Choose My PlateDocumento12 páginasChoose My PlateJose Martinez MoralesAinda não há avaliações
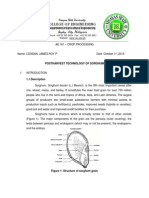
- Postharvest Technology of SorghumDocumento17 páginasPostharvest Technology of SorghumJames RoyAinda não há avaliações
- Finlay MacRitchie - Concepts in Cereal Chemistry-CRC Press (2010) PDFDocumento192 páginasFinlay MacRitchie - Concepts in Cereal Chemistry-CRC Press (2010) PDFEdward PinedaAinda não há avaliações
- NIKOLA TESLA'S Health at 78Documento16 páginasNIKOLA TESLA'S Health at 78Tyler Davis100% (1)
- MVAT Maharashtra VAT Schedule Till 31.3.2016Documento44 páginasMVAT Maharashtra VAT Schedule Till 31.3.2016KevinAinda não há avaliações