Você também pode gostar
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- MENSTRUATION - (NOT) A TABOO - July 3, 4-56 PMDocumento27 páginasMENSTRUATION - (NOT) A TABOO - July 3, 4-56 PMUtkrashtAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- TriageLogic Call Center Policy and Procedure Feb2018 v5.0Documento56 páginasTriageLogic Call Center Policy and Procedure Feb2018 v5.0Nathalie Jane MendozaAinda não há avaliações
- ZhuangZi, Nietzsche, Nature PDFDocumento25 páginasZhuangZi, Nietzsche, Nature PDFJohannes KneslAinda não há avaliações
- History, Examination and Treatment PlaningDocumento78 páginasHistory, Examination and Treatment PlaningShintia HawariAinda não há avaliações
- NCP On Postpartum MotherDocumento9 páginasNCP On Postpartum MotherM.S.H Tube100% (1)
- Archtecture Against The Postpolitical Ed. NadirLahijiDocumento26 páginasArchtecture Against The Postpolitical Ed. NadirLahijiJohannes KneslAinda não há avaliações
- Leigh Brasington: Instruction For Entering JhanaDocumento6 páginasLeigh Brasington: Instruction For Entering JhanaJohannes Knesl100% (3)
- The Work of Andre Green An IntroductionDocumento81 páginasThe Work of Andre Green An IntroductionJohannes KneslAinda não há avaliações
- Wandering and Wonder On Buddhist PathwayDocumento42 páginasWandering and Wonder On Buddhist PathwayJohannes KneslAinda não há avaliações
- WolkenkuckucksheimDocumento2 páginasWolkenkuckucksheimJohannes KneslAinda não há avaliações
- Here Is Looking at You, City of EuropeDocumento112 páginasHere Is Looking at You, City of EuropeJohannes KneslAinda não há avaliações
- Bombay Beach: and So, Acclaimed "Bombay Beach" Starts, and Ends, With This Seminal Sentence: "IDocumento5 páginasBombay Beach: and So, Acclaimed "Bombay Beach" Starts, and Ends, With This Seminal Sentence: "IJohannes KneslAinda não há avaliações
- Remmi DemmiDocumento22 páginasRemmi DemmiJohannes KneslAinda não há avaliações
- LULU. 22.66 77 Spreads To JK 1215, 1216 JKDocumento28 páginasLULU. 22.66 77 Spreads To JK 1215, 1216 JKJohannes KneslAinda não há avaliações
- J. Stone: Some Reflections On Critical BuddhismDocumento30 páginasJ. Stone: Some Reflections On Critical BuddhismJohannes KneslAinda não há avaliações
- Sander Van Maas - Lyrical BodiesDocumento19 páginasSander Van Maas - Lyrical BodiesJohannes KneslAinda não há avaliações
- Laruelle - The Generic As PredicateDocumento34 páginasLaruelle - The Generic As PredicateJohannes Knesl100% (1)
- Dogen and The Unknown KnownsDocumento24 páginasDogen and The Unknown KnownsJohannes KneslAinda não há avaliações
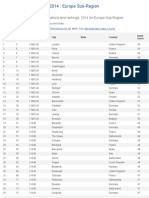
- Innovation Cities™ Index 2014: Europe Sub-Region Innovation Cities Program & Index: City InnovatiDocumento4 páginasInnovation Cities™ Index 2014: Europe Sub-Region Innovation Cities Program & Index: City InnovatiJohannes KneslAinda não há avaliações
- Vax Consent FormDocumento4 páginasVax Consent FormGrace C.Ainda não há avaliações
- Eatern Equatoria State PresentationDocumento24 páginasEatern Equatoria State PresentationMayom MabuongAinda não há avaliações
- Hildebert Wagner, Stefan Kraus, Ksenija Jurcic Auth., Prof. Dr. Dr. H.C. H. Wagner Eds. Immunomodulatory Agents From PlantsDocumento377 páginasHildebert Wagner, Stefan Kraus, Ksenija Jurcic Auth., Prof. Dr. Dr. H.C. H. Wagner Eds. Immunomodulatory Agents From PlantsZafer Corlu100% (1)
- End of LifeDocumento31 páginasEnd of LifeSimran JosanAinda não há avaliações
- Lymphoma HandoutDocumento5 páginasLymphoma Handoutapi-244850728Ainda não há avaliações
- Failure To Thrive With NotesDocumento45 páginasFailure To Thrive With NotesJason Jimmy Lee PillayAinda não há avaliações
- Kolkata HospitalDocumento24 páginasKolkata HospitalKoushikKc ChatterjeeAinda não há avaliações
- 6mins FormDocumento1 página6mins FormPT. Ikenna Kevin EjieloAinda não há avaliações
- Management of Allergic Rhinitis: P. Van Cauwenberge, H. Van HoeckeDocumento20 páginasManagement of Allergic Rhinitis: P. Van Cauwenberge, H. Van HoeckePeter SalimAinda não há avaliações
- Overview of Recommendations For The Uses of Herbal Medicinal Products in The Paediatric PopulationDocumento56 páginasOverview of Recommendations For The Uses of Herbal Medicinal Products in The Paediatric PopulationffkrullAinda não há avaliações
- Case Study Preterm LaborDocumento6 páginasCase Study Preterm LaborAdriane ComaAinda não há avaliações
- Abnormal NipplesDocumento1 páginaAbnormal NipplesdrpamiAinda não há avaliações
- CertificateDocumento1 páginaCertificateDrazarAinda não há avaliações
- Research On Social Work Practice: PurposeDocumento10 páginasResearch On Social Work Practice: PurposeMAHESH KOUJALAGIAinda não há avaliações
- Abbott Alinity S FactSheetDocumento1 páginaAbbott Alinity S FactSheetInayat UllahAinda não há avaliações
- KLP 5 - Nutrition Intake and MedicationDocumento4 páginasKLP 5 - Nutrition Intake and MedicationdzakyAinda não há avaliações
- My Reaction Paper RH Bill (Short)Documento6 páginasMy Reaction Paper RH Bill (Short)Arvee Tee Lodronio60% (5)
- Honest Food GuideDocumento1 páginaHonest Food Guidepeanutmilk100% (3)
- Context Clues Guided Reading 4.1Documento4 páginasContext Clues Guided Reading 4.1Dannah SteeleAinda não há avaliações
- 162 319 1 SMDocumento8 páginas162 319 1 SMAsniar RAinda não há avaliações
- Clinical Questions, PICO, & Study DesignsDocumento3 páginasClinical Questions, PICO, & Study DesignsItan VillalpandoAinda não há avaliações
- Personal Development Plan Learner TemplateDocumento2 páginasPersonal Development Plan Learner TemplateDhaval VaghaniAinda não há avaliações
- Cervical Speculum ExaminationDocumento41 páginasCervical Speculum ExaminationEdwin Delos Reyes AbuAinda não há avaliações
- Adult CardDocumento4 páginasAdult CardagelsantosAinda não há avaliações
- Policies and Procedures Manual Infection Control in General Nursing UnitDocumento9 páginasPolicies and Procedures Manual Infection Control in General Nursing UnitDerick RanaAinda não há avaliações
- Nurs FPX 4020 Assessment 3 Improvement Plan in Service PresentationDocumento6 páginasNurs FPX 4020 Assessment 3 Improvement Plan in Service Presentationzadem5266Ainda não há avaliações