Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Antibiotics - Compleate ClassificationDocumento2 páginasAntibiotics - Compleate ClassificationNeal Gupta83% (12)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- ADHD Medication Chart 2004Documento4 páginasADHD Medication Chart 2004M PatrickAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- EYE DISORDERS GUIDEDocumento115 páginasEYE DISORDERS GUIDEKwabena AmankwaAinda não há avaliações
- Clinical TrialsDocumento39 páginasClinical TrialsYuppie Raj100% (1)
- Regulatory Affairs PDFDocumento12 páginasRegulatory Affairs PDFdrgdsw50% (2)
- Do Not Resuscitate (DNR) ResearchDocumento7 páginasDo Not Resuscitate (DNR) ResearchOmar SalehAinda não há avaliações
- Nursing Care of Patients Undergoing Orthopedic SurgeryDocumento27 páginasNursing Care of Patients Undergoing Orthopedic SurgeryKwabena Amankwa100% (5)
- Preanesthetic Medication JasminaDocumento44 páginasPreanesthetic Medication Jasminaanjali sAinda não há avaliações
- Floating Manipulative TherapyDocumento7 páginasFloating Manipulative TherapyrahmatsahaquillaAinda não há avaliações
- Assignment Writing Guidelines - 2016Documento1 páginaAssignment Writing Guidelines - 2016Kwabena AmankwaAinda não há avaliações
- Muskuoloskeletal System CSDocumento88 páginasMuskuoloskeletal System CSKwabena AmankwaAinda não há avaliações
- New Conceptual Framwork4Documento8 páginasNew Conceptual Framwork4Kwabena AmankwaAinda não há avaliações
- Assignment Writing Guidelines - 2016Documento1 páginaAssignment Writing Guidelines - 2016Kwabena AmankwaAinda não há avaliações
- Anti InfectivesDocumento85 páginasAnti InfectivesKwabena AmankwaAinda não há avaliações
- Current Issues in Health CareDocumento153 páginasCurrent Issues in Health CareKwabena AmankwaAinda não há avaliações
- Where Are The CowriesDocumento19 páginasWhere Are The CowriesKwabena AmankwaAinda não há avaliações
- Where Are The CowriesDocumento19 páginasWhere Are The CowriesKwabena AmankwaAinda não há avaliações
- Employment Considerations: Opportunities, Resumes, & InterviewingDocumento3 páginasEmployment Considerations: Opportunities, Resumes, & InterviewingKwabena AmankwaAinda não há avaliações
- Reflective WritingDocumento3 páginasReflective WritingKwabena AmankwaAinda não há avaliações
- Question Three For BismarkDocumento3 páginasQuestion Three For BismarkKwabena AmankwaAinda não há avaliações
- Reflective WritingDocumento14 páginasReflective WritingKwabena AmankwaAinda não há avaliações
- Vaginal CancerDocumento26 páginasVaginal CancerKwabena AmankwaAinda não há avaliações
- Special Senses PresentationDocumento53 páginasSpecial Senses PresentationKwabena AmankwaAinda não há avaliações
- Human BrainDocumento37 páginasHuman BrainKwabena AmankwaAinda não há avaliações
- Patient Care StudyDocumento49 páginasPatient Care StudyKwabena AmankwaAinda não há avaliações
- New Trends in NursingDocumento111 páginasNew Trends in NursingKwabena AmankwaAinda não há avaliações
- Isaac - Remedial Class Mock Multiple ChoiceDocumento12 páginasIsaac - Remedial Class Mock Multiple ChoiceKwabena AmankwaAinda não há avaliações
- Fred (1-5) (1) Final MarkingDocumento51 páginasFred (1-5) (1) Final MarkingKwabena AmankwaAinda não há avaliações
- BPH PresentationDocumento33 páginasBPH PresentationKwabena AmankwaAinda não há avaliações
- Nutritional AnemiaDocumento19 páginasNutritional AnemiaKwabena AmankwaAinda não há avaliações
- BPH PresentationDocumento33 páginasBPH PresentationKwabena AmankwaAinda não há avaliações
- Femur fracture assessment and treatment exam questionsDocumento8 páginasFemur fracture assessment and treatment exam questionsKwabena Amankwa100% (2)
- Five Rights of Drug Admin PowerpointDocumento32 páginasFive Rights of Drug Admin PowerpointManoj KumarAinda não há avaliações
- Chapter OneDocumento49 páginasChapter OneKwabena AmankwaAinda não há avaliações
- Research Methodology - IIIDocumento337 páginasResearch Methodology - IIIKwabena AmankwaAinda não há avaliações
- Oncology 2Documento128 páginasOncology 2Kwabena AmankwaAinda não há avaliações
- ADRENEGICSDocumento32 páginasADRENEGICSKwabena AmankwaAinda não há avaliações
- Clobazam Thame 5mg/5ml and 10mg/5ml Oral Suspension PARDocumento22 páginasClobazam Thame 5mg/5ml and 10mg/5ml Oral Suspension PARHemang M. GajjarAinda não há avaliações
- Medication Errors: BY DR - Divya Ashok Kulkarni. Pharm DDocumento68 páginasMedication Errors: BY DR - Divya Ashok Kulkarni. Pharm DShrenil LagadAinda não há avaliações
- Colchicine drug information and nursing implicationsDocumento3 páginasColchicine drug information and nursing implicationsTri Purma SariAinda não há avaliações
- Panadol Paracetamol: Medical UseDocumento5 páginasPanadol Paracetamol: Medical UseAbdelrhman AboodaAinda não há avaliações
- Kelly Et Al-2015-Journal of Clinical Pharmacy and TherapeuticsDocumento7 páginasKelly Et Al-2015-Journal of Clinical Pharmacy and TherapeuticsmaleticjAinda não há avaliações
- Marikina Drug Symposium Highlights Dangers of Shabu, Marijuana and InhalantsDocumento2 páginasMarikina Drug Symposium Highlights Dangers of Shabu, Marijuana and InhalantsLoeyAinda não há avaliações
- Geri ScriptDocumento172 páginasGeri Scriptmmeisels257100% (1)
- Tricyclic antidepressants overviewDocumento2 páginasTricyclic antidepressants overviewAaLona RobinsonAinda não há avaliações
- Vastarel MR 35mgDocumento1 páginaVastarel MR 35mgPhil Edgar Contreras RNAinda não há avaliações
- Lesson Plan 5 Medicine LabelDocumento35 páginasLesson Plan 5 Medicine Labelnta tiekaAinda não há avaliações
- AnalgesicDrugs Combinations in Thetreatment of Different Types of PainDocumento68 páginasAnalgesicDrugs Combinations in Thetreatment of Different Types of PainAnuj MairhAinda não há avaliações
- Absorption and Half-Life: Nick Holford Dept Pharmacology & Clinical Pharmacology University of Auckland, New ZealandDocumento7 páginasAbsorption and Half-Life: Nick Holford Dept Pharmacology & Clinical Pharmacology University of Auckland, New ZealandkbnarkhedeAinda não há avaliações
- Principle of Drug ActionDocumento4 páginasPrinciple of Drug ActionChristopher jan LegaspiAinda não há avaliações
- IMS Oncology Trend Report 2017 Advances Complexity CostDocumento47 páginasIMS Oncology Trend Report 2017 Advances Complexity CostEkta Dhawan RampalAinda não há avaliações
- Sif ReportDocumento15 páginasSif ReportMANISH NIGAMAinda não há avaliações
- PME Feb.Documento52 páginasPME Feb.Fernando ComasAinda não há avaliações
- Jacob ExcelDocumento8 páginasJacob ExcelPeter KiruiAinda não há avaliações
- MJV2Documento2 páginasMJV2Mervin BocatcatAinda não há avaliações
- Epistatus EpilepsijaDocumento3 páginasEpistatus Epilepsijacards_2Ainda não há avaliações
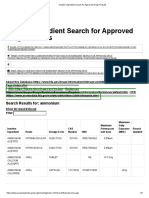
- Inactive Ingredient Search For Approved Drug ProductsDocumento3 páginasInactive Ingredient Search For Approved Drug ProductsDang Chi CongAinda não há avaliações
- Obs and dlt-1Documento74 páginasObs and dlt-1paru100% (1)
- Antifungal Drugs: University of Nairobi Department of Public Health, Pharmacology & ToxicologyDocumento32 páginasAntifungal Drugs: University of Nairobi Department of Public Health, Pharmacology & ToxicologyAnonymous RA6sVagiAinda não há avaliações
- Medication Safety in LactationDocumento30 páginasMedication Safety in Lactationhalima alzadjaliAinda não há avaliações