Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Hemodialysis Patient's Endorsement FormDocumento1 páginaHemodialysis Patient's Endorsement FormHacienda Galea Resort and Events Place100% (1)
- Appendix 3 Examples of Dilutions of Anaesthetic Mixtures For Small Rodents 2016 Laboratory Animal Anaesthesia Fourth EditionDocumento4 páginasAppendix 3 Examples of Dilutions of Anaesthetic Mixtures For Small Rodents 2016 Laboratory Animal Anaesthesia Fourth EditionAlejandra CárdenasAinda não há avaliações
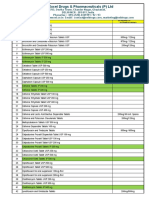
- Generic Medicines PricelistDocumento15 páginasGeneric Medicines PricelistJoseph Michael Vitug100% (1)
- Activity 6 Online Resources RetrievalDocumento4 páginasActivity 6 Online Resources RetrievalHazel Jane AquinoAinda não há avaliações
- Extravasation Management ProtocolDocumento1 páginaExtravasation Management ProtocolThắng NguyễnAinda não há avaliações
- Session 08 EctDocumento23 páginasSession 08 EctMalakatete Mwaipojele-fAinda não há avaliações
- Medisiddh Pharma Private Limited 971A/6, Thirumal Nagar, Near K.R Arts College-Nh7, Kovilpatti-628503 LICENSE NO: 490/25DDocumento2 páginasMedisiddh Pharma Private Limited 971A/6, Thirumal Nagar, Near K.R Arts College-Nh7, Kovilpatti-628503 LICENSE NO: 490/25Dhk_scribdAinda não há avaliações
- TDM of Valproic AcidDocumento43 páginasTDM of Valproic Acidryo_ninukAinda não há avaliações
- Barcode List FinalDocumento6 páginasBarcode List FinalMhammad NaveedAinda não há avaliações
- QRG Morpheus8 BODY February 2021 (TIPS)Documento2 páginasQRG Morpheus8 BODY February 2021 (TIPS)JWAinda não há avaliações
- Care Homes - Good Practice Guidance Expiry Dates For MedicationDocumento1 páginaCare Homes - Good Practice Guidance Expiry Dates For MedicationafrizalsyahyeriAinda não há avaliações
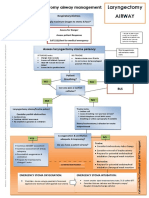
- Laryngectomy Airway: Emergency Tracheostomy Airway ManagementDocumento1 páginaLaryngectomy Airway: Emergency Tracheostomy Airway ManagementDana IlieAinda não há avaliações
- Inform Concent Actemra 1Documento2 páginasInform Concent Actemra 1lukiharjantiAinda não há avaliações
- RJPDocumento38 páginasRJPjoyfullAinda não há avaliações
- Major and Minor TranquilizerDocumento6 páginasMajor and Minor TranquilizerAli IjazAinda não há avaliações
- JunaidDocumento41 páginasJunaidShobhit GoswamiAinda não há avaliações
- Case 11 J&J Again Recalls Thousands of Faulty Hip ImplantsDocumento2 páginasCase 11 J&J Again Recalls Thousands of Faulty Hip ImplantsShiela Mae Catalan AludoAinda não há avaliações
- Flix o Tide InhalerDocumento5 páginasFlix o Tide InhalerEthik MoesAinda não há avaliações
- Campral (Acamprosate Calcium)Documento1 páginaCampral (Acamprosate Calcium)E100% (1)
- Route of Administration PDFDocumento45 páginasRoute of Administration PDFBurhan MubasharAinda não há avaliações
- Before Taking Losartan,: What Special Dietary Instructions Should I Follow?Documento8 páginasBefore Taking Losartan,: What Special Dietary Instructions Should I Follow?Hillary Ann AbuelAinda não há avaliações
- Drug Interaction MonitoringDocumento5 páginasDrug Interaction MonitoringAnonymousAinda não há avaliações
- Routes of Drug AdministrationDocumento34 páginasRoutes of Drug AdministrationNa SyaAinda não há avaliações
- Nacromin Eye DropsDocumento2 páginasNacromin Eye DropsAnamul hossainAinda não há avaliações
- Test Bank For Drug Calculations Ratio and Proportion Problems For Clinical Practice 9th Edition BrownDocumento19 páginasTest Bank For Drug Calculations Ratio and Proportion Problems For Clinical Practice 9th Edition BrownGraceLopezyfmox100% (37)
- Successful Treatment of Amoxapine Induced IntractaDocumento5 páginasSuccessful Treatment of Amoxapine Induced IntractaNatasha Vera100% (1)
- New Checklist Trolley Emergency Icu Revisi 12 Okt 2021Documento4 páginasNew Checklist Trolley Emergency Icu Revisi 12 Okt 2021Laras TriAinda não há avaliações
- Rituximab TrialDocumento9 páginasRituximab TrialsrildaAinda não há avaliações
- A Guide To Calculating Parenteral Nutrition When T-2 - 1Documento2 páginasA Guide To Calculating Parenteral Nutrition When T-2 - 1Steve JacobAinda não há avaliações
- VXL-List of Pharma Products (Domestic and Export)Documento10 páginasVXL-List of Pharma Products (Domestic and Export)Singh PushpanjaliAinda não há avaliações