Você também pode gostar
- Quality of Vision (Essential Optics)Documento142 páginasQuality of Vision (Essential Optics)SmaraAinda não há avaliações
- Impact of Intraocular Lens Haptic Design and OrientationDocumento19 páginasImpact of Intraocular Lens Haptic Design and Orientationvictor_napitupuluAinda não há avaliações
- OrthopticDocumento9 páginasOrthopticSobiafarooqAinda não há avaliações
- Dispensing NotesDocumento103 páginasDispensing Notesjancok100% (1)
- Eye ExaminationDocumento6 páginasEye ExaminationChellamani UmakanthanAinda não há avaliações
- Optometry Department OPTO 374 The Synoptophore Dr. Safiah Mulla Name: Fatima Ahmad Abo-Qoaied ID: 426200452Documento25 páginasOptometry Department OPTO 374 The Synoptophore Dr. Safiah Mulla Name: Fatima Ahmad Abo-Qoaied ID: 426200452zecemariAinda não há avaliações
- Refraction and PrescribingDocumento6 páginasRefraction and PrescribingawaisAinda não há avaliações
- Visual Field TestingDocumento16 páginasVisual Field TestingHendry HuangAinda não há avaliações
- (Optical Sciences and Applications of Light) Sun, Haiyin - Lens Design - A Practical guide-CRC Press (2017)Documento374 páginas(Optical Sciences and Applications of Light) Sun, Haiyin - Lens Design - A Practical guide-CRC Press (2017)Vivian Amos100% (1)
- Understanding Aberrometry for Eye CareDocumento54 páginasUnderstanding Aberrometry for Eye Caresightbd100% (2)
- 03 Refractive SurgeryDocumento99 páginas03 Refractive SurgeryWaqar Ahmad Khan100% (3)
- Aspheric IOLs Fact vs MythDocumento8 páginasAspheric IOLs Fact vs MythAnonymous h0DxuJTAinda não há avaliações
- Ophthalmology Femtosecond LaserDocumento8 páginasOphthalmology Femtosecond LaserChandrika MaluftiAinda não há avaliações
- Eye Docs StrabismusDocumento121 páginasEye Docs StrabismusMuneeb ShahzadAinda não há avaliações
- British Orthoptic Journal 2002Documento9 páginasBritish Orthoptic Journal 2002roelkloosAinda não há avaliações
- Clinical Study: Aspheric Intraocular Lenses Implantation For Cataract Patients With Extreme MyopiaDocumento6 páginasClinical Study: Aspheric Intraocular Lenses Implantation For Cataract Patients With Extreme MyopiaKevin ArdiansyahAinda não há avaliações
- High Myopiaypartial Reduction Ortho-K: A 2-Year Randomized StudyDocumento10 páginasHigh Myopiaypartial Reduction Ortho-K: A 2-Year Randomized StudykarakuraAinda não há avaliações
- Dynamic RetinosDocumento6 páginasDynamic RetinosguybarnettAinda não há avaliações
- StrabismusDocumento9 páginasStrabismuspandejuniartaAinda não há avaliações
- The Effects of Glasses For Anisometropia On Stereopsis: Kimleejy@hallym - Or.krDocumento7 páginasThe Effects of Glasses For Anisometropia On Stereopsis: Kimleejy@hallym - Or.krpoetraAinda não há avaliações
- The Ocular Biometric and Corneal Topographic Characteristics of High-Anisometropic Adults in TaiwanDocumento6 páginasThe Ocular Biometric and Corneal Topographic Characteristics of High-Anisometropic Adults in TaiwanNurul Falah KalokoAinda não há avaliações
- High Myopia and Glaucoma Susceptibility The Beijing Eye StudyDocumento5 páginasHigh Myopia and Glaucoma Susceptibility The Beijing Eye StudyDickyStevanoZukhriAinda não há avaliações
- 646-Article Text-2088-1-2-20190613Documento9 páginas646-Article Text-2088-1-2-20190613Faradiba NoviandiniAinda não há avaliações
- IndianJOphthalmol624461-9214366 023334Documento3 páginasIndianJOphthalmol624461-9214366 023334secret_sunsetAinda não há avaliações
- How Far Is Observation Allowed in Patients With Ectopia Lentis?Documento8 páginasHow Far Is Observation Allowed in Patients With Ectopia Lentis?Syeda F AmbreenAinda não há avaliações
- Clinical OpticDocumento43 páginasClinical OpticReinhard TuerahAinda não há avaliações
- Voluntary Effort As A Stimulus To Accommodation and VergenceDocumento8 páginasVoluntary Effort As A Stimulus To Accommodation and VergenceRicardo BarretoAinda não há avaliações
- Um Estudo Da Visualização Excêntrico Formação para Baixa Visão ReabilitaçãoDocumento8 páginasUm Estudo Da Visualização Excêntrico Formação para Baixa Visão ReabilitaçãoEduardo VieiraAinda não há avaliações
- Intraindividual Comparison of Aspherical and Spherical Intraocular Lenses of Same Material and PlatformDocumento6 páginasIntraindividual Comparison of Aspherical and Spherical Intraocular Lenses of Same Material and PlatformAkhilesh KumarAinda não há avaliações
- Retinal Image Quality of A Human Eye Model - OSLO LT SoftwareDocumento11 páginasRetinal Image Quality of A Human Eye Model - OSLO LT SoftwareRadu BabauAinda não há avaliações
- Effect of Ocular Dominance On The Latency and Amplitude of Visual Evoked PotentialsDocumento6 páginasEffect of Ocular Dominance On The Latency and Amplitude of Visual Evoked PotentialsMaria FernandaAinda não há avaliações
- PIIS0002939422004184Documento7 páginasPIIS0002939422004184Anca Florina GaceaAinda não há avaliações
- Accepted Manuscript: 10.1016/j.jaapos.2017.05.009Documento19 páginasAccepted Manuscript: 10.1016/j.jaapos.2017.05.009Lingesh 2813Ainda não há avaliações
- Anomalous Retinal Correspondence - Diagnostic Tests and TherapyDocumento5 páginasAnomalous Retinal Correspondence - Diagnostic Tests and TherapySumon SarkarAinda não há avaliações
- The Analysis of AC/A Ratio in Nonrefractive Accommodative Esotropia Treated With Bifocal GlassesDocumento6 páginasThe Analysis of AC/A Ratio in Nonrefractive Accommodative Esotropia Treated With Bifocal GlassesTimbul SianturiAinda não há avaliações
- Contact Lenses Vs Spectacles in Myopes: Is There Any Difference in Accommodative and Binocular Function?Documento12 páginasContact Lenses Vs Spectacles in Myopes: Is There Any Difference in Accommodative and Binocular Function?mau tauAinda não há avaliações
- Errors of Refraction - Presbyopia, AstigmatismDocumento16 páginasErrors of Refraction - Presbyopia, AstigmatismVid MirosevicAinda não há avaliações
- Indirect OphthalmosDocumento3 páginasIndirect Ophthalmosbijujc100% (1)
- Jurnal MataDocumento7 páginasJurnal Matahelmi luthfiAinda não há avaliações
- SCORM Lens Power Paper 2012Documento7 páginasSCORM Lens Power Paper 2012Rafael IribarrenAinda não há avaliações
- Supperssion Eye Movements Improves BalanceDocumento7 páginasSupperssion Eye Movements Improves BalanceKhaled AbuzayanAinda não há avaliações
- AncdDocumento7 páginasAncdNurulia RizkiAinda não há avaliações
- Fundoscopy GuideDocumento10 páginasFundoscopy Guidedrjanggeum0% (1)
- Cycloplegic Effect of 0.5%tropicamide and 0.5%phenylephrine Mixed Eye Drops - Objective Assessment in Japanese Schoolchildren With MyopiaDocumento5 páginasCycloplegic Effect of 0.5%tropicamide and 0.5%phenylephrine Mixed Eye Drops - Objective Assessment in Japanese Schoolchildren With Myopiaal_dhi_01Ainda não há avaliações
- AstigmatismDocumento29 páginasAstigmatismAmjad bbsulkAinda não há avaliações
- Influence of Postoperative Astigmatism On Uncorrected Near Visual Acuity in PseudophakiaDocumento7 páginasInfluence of Postoperative Astigmatism On Uncorrected Near Visual Acuity in PseudophakiaIJAR JOURNALAinda não há avaliações
- 3585 6756 1 SM PDFDocumento7 páginas3585 6756 1 SM PDFYolanda Rinarti RakaAinda não há avaliações
- 13 Subjective RefractionDocumento19 páginas13 Subjective Refractionmuhammad farizAinda não há avaliações
- Visual Outcomes and Complications of Piggyback Intraocular Lens Implantation Compared To Aphakia For Infantile CataractDocumento8 páginasVisual Outcomes and Complications of Piggyback Intraocular Lens Implantation Compared To Aphakia For Infantile CataractElyani RahmanAinda não há avaliações
- Examination of The RetinaDocumento3 páginasExamination of The RetinaGus LionsAinda não há avaliações
- Quantitative Assessment of Inferior Oblique Muscle Overaction Using Photographs of The Cardinal Positions of GazeDocumento9 páginasQuantitative Assessment of Inferior Oblique Muscle Overaction Using Photographs of The Cardinal Positions of GazenysAinda não há avaliações
- Myopia Control During Orthokeratology Lens Wear in Children Using A Novel Study DesignDocumento11 páginasMyopia Control During Orthokeratology Lens Wear in Children Using A Novel Study DesignLisa WidiasmokoAinda não há avaliações
- Original Article: The Effect of Experimentally Induced Anisometropia On Binocularity and Bifoveal FixationDocumento7 páginasOriginal Article: The Effect of Experimentally Induced Anisometropia On Binocularity and Bifoveal FixationNurul Falah KalokoAinda não há avaliações
- Jurnal MataDocumento7 páginasJurnal MatafaniaapriskaAinda não há avaliações
- Literature Review of Refractive ErrorDocumento7 páginasLiterature Review of Refractive Errorafdtsdece100% (1)
- Higher Order Aberration and Astigmatism in Children With Hyperopic AmblyopiaDocumento7 páginasHigher Order Aberration and Astigmatism in Children With Hyperopic AmblyopiaEko WidayantoAinda não há avaliações
- Imbatranire CristalinDocumento8 páginasImbatranire CristalinGeanina GulutaAinda não há avaliações
- Evaluation of Relationship of Ocular Parameters and Depth of Anisometropic Amblyopia With The Degree of AnisometropiaDocumento5 páginasEvaluation of Relationship of Ocular Parameters and Depth of Anisometropic Amblyopia With The Degree of AnisometropiaGitaAinda não há avaliações
- Ocular Emergencies 2017Documento18 páginasOcular Emergencies 2017Sebastian BarreraAinda não há avaliações
- Comparison of The Effect of Cycloplegia On Astigmatism Measurement in A Pediatric Amblyopic PopulationDocumento6 páginasComparison of The Effect of Cycloplegia On Astigmatism Measurement in A Pediatric Amblyopic PopulationSyaiful UlumAinda não há avaliações
- Atropine Treatment of Amblyopia: Is A Swap in Fixation Necessary?Documento10 páginasAtropine Treatment of Amblyopia: Is A Swap in Fixation Necessary?heartless_nobodiAinda não há avaliações
- Cycloplegic Refraction in AdultDocumento50 páginasCycloplegic Refraction in AdultShahid ManzoorAinda não há avaliações
- Briici Ner Test: Andrea Cibis Tongue, Gerhard W. CibistDocumento4 páginasBriici Ner Test: Andrea Cibis Tongue, Gerhard W. CibistAgam Bhandari ( RPC)Ainda não há avaliações
- IOL Power Calculation, Correction of Defocus - CH 4Documento18 páginasIOL Power Calculation, Correction of Defocus - CH 4riveliAinda não há avaliações
- OCULOPATHY - Disproves the orthodox and theoretical bases upon which glasses are so freely prescribed, and puts forward natural remedial methods of treatment for what are sometimes termed incurable visual defectsNo EverandOCULOPATHY - Disproves the orthodox and theoretical bases upon which glasses are so freely prescribed, and puts forward natural remedial methods of treatment for what are sometimes termed incurable visual defectsAinda não há avaliações
- Mata36a PDFDocumento10 páginasMata36a PDFIndra PermanaAinda não há avaliações
- Initial Resus TableDocumento3 páginasInitial Resus TableParama AdhikresnaAinda não há avaliações
- KP LamafIS Sin1Documento1 páginaKP LamafIS Sin1Indra PermanaAinda não há avaliações
- Jurnal Mata PonkoppDocumento7 páginasJurnal Mata PonkoppIndra PermanaAinda não há avaliações
- Journal LL LL PediatriDocumento4 páginasJournal LL LL PediatriIndra PermanaAinda não há avaliações
- Jurnal ObgynDocumento10 páginasJurnal ObgynIndra PermanaAinda não há avaliações
- Anti Vegf Drugs in The Prevention of BlindnessDocumento3 páginasAnti Vegf Drugs in The Prevention of BlindnessIndra PermanaAinda não há avaliações
- Daftar PusTaka SNHDocumento7 páginasDaftar PusTaka SNHIndra PermanaAinda não há avaliações
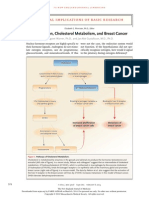
- CholesterolDocumento2 páginasCholesterolIndra PermanaAinda não há avaliações
- Abnormal Breath SoundsDocumento3 páginasAbnormal Breath SoundsIndra PermanaAinda não há avaliações
- Metodologi Penelitian Kedokteran Dan Kesehatan Kedokteran Dan KesehatanDocumento16 páginasMetodologi Penelitian Kedokteran Dan Kesehatan Kedokteran Dan KesehatanGhisqy Arsy MulkiAinda não há avaliações
- Wrap Up Skenario 1 Pilek Pagi Hari Blok Sistem RespirasiDocumento1 páginaWrap Up Skenario 1 Pilek Pagi Hari Blok Sistem RespirasiIndra PermanaAinda não há avaliações
- Penggunaan Berbagai Cut-Off Indeks Massa Tubuh Sebagai Indikator Obesitas Terkait Penyakit Degeneratif Di IndonesiaDocumento14 páginasPenggunaan Berbagai Cut-Off Indeks Massa Tubuh Sebagai Indikator Obesitas Terkait Penyakit Degeneratif Di IndonesiaLutfi RensiansiAinda não há avaliações
- Abnormal Breath SoundsDocumento3 páginasAbnormal Breath SoundsIndra PermanaAinda não há avaliações
- Intraindividual Comparison of Aspherical and Spherical Intraocular Lenses of Same Material and PlatformDocumento6 páginasIntraindividual Comparison of Aspherical and Spherical Intraocular Lenses of Same Material and PlatformAkhilesh KumarAinda não há avaliações
- Book Chapter Physiology of Astigmatism 2012Documento20 páginasBook Chapter Physiology of Astigmatism 2012Sebas H. MonsalveAinda não há avaliações
- Oculus: Pentacam Pentacam HRDocumento20 páginasOculus: Pentacam Pentacam HRSaecio OpticoAinda não há avaliações
- Hill IQ PreferenceDocumento4 páginasHill IQ PreferencefdoaguayoAinda não há avaliações
- Pearls For Implantable Phakic Contact Lens (Care Group India) by DR Suresh K Pandey DR Vidushi Sharma, SuVi Eye Institute Kota IndiaDocumento66 páginasPearls For Implantable Phakic Contact Lens (Care Group India) by DR Suresh K Pandey DR Vidushi Sharma, SuVi Eye Institute Kota IndiaDr Suresh K Pandey100% (1)
- Brochure - STAAR Surgical - EVO Visian ICL (Surgeon Brochure) (En)Documento12 páginasBrochure - STAAR Surgical - EVO Visian ICL (Surgeon Brochure) (En)Andreea L. MihalceaAinda não há avaliações
- Chromatic Aberration: Basic Optics, Chapter 26Documento63 páginasChromatic Aberration: Basic Optics, Chapter 26PAM ALVARADOAinda não há avaliações
- Contact Lenses Resource Guide: ConnectionDocumento44 páginasContact Lenses Resource Guide: ConnectionproxyAinda não há avaliações
- GALILEI Map Interpretation GuideDocumento98 páginasGALILEI Map Interpretation GuideShi Ying0% (1)
- I.scription ECP BrochureDocumento4 páginasI.scription ECP BrochureZenithashAinda não há avaliações
- Pentacam en PDFDocumento20 páginasPentacam en PDFvictorAinda não há avaliações
- Aio Vol 1 Issue 1 Sep 2013Documento56 páginasAio Vol 1 Issue 1 Sep 2013aiojournalAinda não há avaliações
- Aao Irregular AstigmatismDocumento16 páginasAao Irregular AstigmatismnurulrezqiaAinda não há avaliações
- Unilateral Miopia KarenaDocumento4 páginasUnilateral Miopia KarenaHardina Yusri ChanAinda não há avaliações
- 2008 - Irregular - Astigmatism - Diagnosis - (Ming - Wang - MD) - PDFDocumento606 páginas2008 - Irregular - Astigmatism - Diagnosis - (Ming - Wang - MD) - PDFRuslan IshalAinda não há avaliações
- Pentacam enDocumento18 páginasPentacam endarkspawn69Ainda não há avaliações
- Essilor VariluxDocumento53 páginasEssilor VariluxBdv RaoAinda não há avaliações
- Pentcam 5tDocumento16 páginasPentcam 5tMarian FasieAinda não há avaliações
- The Optical Design of The Human Eye: A Critical ReviewDocumento16 páginasThe Optical Design of The Human Eye: A Critical ReviewAna LabeAinda não há avaliações
- Fem To Second LaserDocumento4 páginasFem To Second LaserIlham Suryo Wibowo AntonoAinda não há avaliações
- ADVANCED MEDICAL OPTICS INC 10-K (Annual Reports) 2009-02-24Documento212 páginasADVANCED MEDICAL OPTICS INC 10-K (Annual Reports) 2009-02-24http://secwatch.com100% (4)
- Aladdin 3.0 BrochureDocumento16 páginasAladdin 3.0 Brochuredarkspawn69Ainda não há avaliações
- Schwind Cam Perfect Planning - Wide Range of Applications: Ork-Cam Presbymax Ptk-CamDocumento8 páginasSchwind Cam Perfect Planning - Wide Range of Applications: Ork-Cam Presbymax Ptk-CamThales FerreiraAinda não há avaliações
- I TraceDocumento38 páginasI TraceShahad Ismael100% (1)
- A Randomised, Prospective Study To Investigate The Efficacy of Riboflavinultraviolet A 370 NM Coroneal Collagen Cross Linkage To Halt The Progression of KeratoconusDocumento7 páginasA Randomised, Prospective Study To Investigate The Efficacy of Riboflavinultraviolet A 370 NM Coroneal Collagen Cross Linkage To Halt The Progression of Keratoconusurs lovinglyAinda não há avaliações