Você também pode gostar
- Prevalence of Irritable Bowel Syndrome in Caregivers of Patients With Chronic DiseasesDocumento8 páginasPrevalence of Irritable Bowel Syndrome in Caregivers of Patients With Chronic Diseasesapi-193771047Ainda não há avaliações
- Irritable Bowel Syndrome: Physicians' Awareness and Patients' ExperienceDocumento6 páginasIrritable Bowel Syndrome: Physicians' Awareness and Patients' Experienceapi-193771047Ainda não há avaliações
- Partner Burden in Irritable Bowel Syndrome: See Editorial On Page 156Documento5 páginasPartner Burden in Irritable Bowel Syndrome: See Editorial On Page 156api-193771047Ainda não há avaliações
- Anxiety-Depressive Disorders Among Irritable Bowel Syndrome Patients in Guilan, IranDocumento7 páginasAnxiety-Depressive Disorders Among Irritable Bowel Syndrome Patients in Guilan, Iranapi-193771047Ainda não há avaliações
- Anxiety, Stress, & Coping: An International JournalDocumento17 páginasAnxiety, Stress, & Coping: An International Journalapi-193771047Ainda não há avaliações
- Health Effects of Expressive Letter Writing: Mosher and Danoff-BurgDocumento19 páginasHealth Effects of Expressive Letter Writing: Mosher and Danoff-Burgapi-193771047Ainda não há avaliações
- Behaviour Research and TherapyDocumento9 páginasBehaviour Research and Therapyapi-193771047Ainda não há avaliações
- Healing Words: Using Affect Labeling To Reduce The Effects of Unpleasant Cues On Symptom Reporting in IBS PatientsDocumento9 páginasHealing Words: Using Affect Labeling To Reduce The Effects of Unpleasant Cues On Symptom Reporting in IBS Patientsapi-193771047Ainda não há avaliações
- Health Psychology Review: Click For UpdatesDocumento25 páginasHealth Psychology Review: Click For Updatesapi-193771047Ainda não há avaliações
- Original Papers: The Lifetime Prevalence of Anxiety Disorders Among Patients With Irritable Bowel SyndromeDocumento6 páginasOriginal Papers: The Lifetime Prevalence of Anxiety Disorders Among Patients With Irritable Bowel Syndromeapi-193771047Ainda não há avaliações
- Autonomic Effects of Expressive Writing in Individuals With Elevated Blood PressureDocumento13 páginasAutonomic Effects of Expressive Writing in Individuals With Elevated Blood Pressureapi-193771047Ainda não há avaliações
- Illness Perceptions Mediate The Relationship Between Bowel Symptom Severity and Health-Related Quality of Life in IBS PatientsDocumento12 páginasIllness Perceptions Mediate The Relationship Between Bowel Symptom Severity and Health-Related Quality of Life in IBS Patientsapi-193771047Ainda não há avaliações
- Does Expressive Writing Reduce Stress and Improve Health For Family Caregivers of Older Adults?Documento11 páginasDoes Expressive Writing Reduce Stress and Improve Health For Family Caregivers of Older Adults?api-193771047Ainda não há avaliações
- Feature: Biofeedback and Expressive Writing: Emotional Disclosure and Its Effects On HealthDocumento6 páginasFeature: Biofeedback and Expressive Writing: Emotional Disclosure and Its Effects On Healthapi-193771047Ainda não há avaliações
- In Search of Attachment: A Qualitative Study of Chronically Ill Women Transitioning Between Family Physicians in Rural Ontario, CanadaDocumento12 páginasIn Search of Attachment: A Qualitative Study of Chronically Ill Women Transitioning Between Family Physicians in Rural Ontario, Canadaapi-193771047Ainda não há avaliações
- Learning About Oneself Through Others: Experiences of A Group-Based Patient Education Programme About Irritable Bowel SyndromeDocumento10 páginasLearning About Oneself Through Others: Experiences of A Group-Based Patient Education Programme About Irritable Bowel Syndromeapi-193771047Ainda não há avaliações
- Psychodynamic Interpersonal Therapy and Improvement in Interpersonal Difficulties in People With Severe Irritable Bowel SyndromeDocumento8 páginasPsychodynamic Interpersonal Therapy and Improvement in Interpersonal Difficulties in People With Severe Irritable Bowel Syndromeapi-193771047Ainda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- ISBDFinal Book 2012 BDocumento53 páginasISBDFinal Book 2012 BvadamadaAinda não há avaliações
- The NysseDocumento208 páginasThe NysseSiti Nur JariyahAinda não há avaliações
- C1 Ob-Gyn-2020Documento33 páginasC1 Ob-Gyn-2020yabsera mulatuAinda não há avaliações
- Mentha Cordifelia TeaDocumento10 páginasMentha Cordifelia TeaMia Pearl Tabios ValenzuelaAinda não há avaliações
- Icpc 2 R PDFDocumento204 páginasIcpc 2 R PDFagni sukma fahiraAinda não há avaliações
- 0-0013 PDFDocumento24 páginas0-0013 PDFisabellaprie3Ainda não há avaliações
- Sample Only - Not For Clinical UseDocumento6 páginasSample Only - Not For Clinical Usenostra83Ainda não há avaliações
- CV - Microbiology Infection ControlDocumento14 páginasCV - Microbiology Infection ControlDrRahul KambleAinda não há avaliações
- Evedenced Based Rectal ProlapseDocumento16 páginasEvedenced Based Rectal Prolapsesub_zero9909Ainda não há avaliações
- II-E Altered PerceptionDocumento16 páginasII-E Altered PerceptionDharylle CariñoAinda não há avaliações
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Documento2 páginasIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Recruitment Cell Aiims BilaspurAinda não há avaliações
- Pap SmearDocumento75 páginasPap SmearRaine BowAinda não há avaliações
- Geriatric NursingDocumento64 páginasGeriatric NursingMark Elben100% (2)
- Takayasu S Arter It IsDocumento5 páginasTakayasu S Arter It IsButarbutar MelvaAinda não há avaliações
- Cholinergic SyndromeDocumento3 páginasCholinergic SyndromeEmman AguilarAinda não há avaliações
- (2020) (Libro) Health Psychology - The BasicsDocumento267 páginas(2020) (Libro) Health Psychology - The BasicsERIKA REYES GOMEZAinda não há avaliações
- 11 - Precautions For Handling Organic SolventDocumento2 páginas11 - Precautions For Handling Organic SolventMummy TheAinda não há avaliações
- Dr. Ernst Ziegler-1stEd PDFDocumento392 páginasDr. Ernst Ziegler-1stEd PDFcasAinda não há avaliações
- 3 Minute Exam DFSDocumento2 páginas3 Minute Exam DFSWeeChuan NgAinda não há avaliações
- Buildings and Structures: Padua EsteDocumento2 páginasBuildings and Structures: Padua EsteKevin LavinaAinda não há avaliações
- 1-Disease MechanismsDocumento5 páginas1-Disease MechanismsMarian Dane PunzalanAinda não há avaliações
- Clonazepam Drug CardDocumento1 páginaClonazepam Drug CardSheri490Ainda não há avaliações
- Sarcoidosis Pathophysiology, Diagnosis AtfDocumento6 páginasSarcoidosis Pathophysiology, Diagnosis AtfpatriciaAinda não há avaliações
- Chest Physician in Pune - Dr. Sharadchandra YadavDocumento8 páginasChest Physician in Pune - Dr. Sharadchandra YadavSharad YadavAinda não há avaliações
- Classical Western FormulasDocumento4 páginasClassical Western FormulasSofia MirandaAinda não há avaliações
- RANZCPdepression 2Documento120 páginasRANZCPdepression 2Random_EggAinda não há avaliações
- CASE PRESENTATION NEPHROTIC Syndrome-1Documento20 páginasCASE PRESENTATION NEPHROTIC Syndrome-1rohankananiAinda não há avaliações
- 2.1 NCM 109 - Pregestational ConditionsDocumento6 páginas2.1 NCM 109 - Pregestational ConditionsSittie Haneen TabaraAinda não há avaliações
- Panadeine: What Is in This LeafletDocumento3 páginasPanadeine: What Is in This Leafletradzi66Ainda não há avaliações
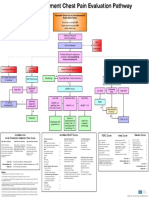
- Emergency Department Chest Pain Evaluation PathwayDocumento2 páginasEmergency Department Chest Pain Evaluation Pathwaymuhammad sajidAinda não há avaliações