Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Pediatric Critical Care Nutrition PDFDocumento324 páginasPediatric Critical Care Nutrition PDFNia DefinisiAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Metabolic Interrelationships Rev 07-11-2014Documento82 páginasMetabolic Interrelationships Rev 07-11-2014algutAinda não há avaliações
- Prodew 400: Amino Acid Based Humectant For Skin CareDocumento26 páginasProdew 400: Amino Acid Based Humectant For Skin CareKlara Miliktrisa KirbitievnaAinda não há avaliações
- 1964 Death and Disease in Infants and Toddlers of Preindustrial Countries. AJPHNHDocumento6 páginas1964 Death and Disease in Infants and Toddlers of Preindustrial Countries. AJPHNHChristine ChambersAinda não há avaliações
- Metabolic Screening in Children Newborn ScreeningDocumento6 páginasMetabolic Screening in Children Newborn ScreeningJohn Lemuel GuevarraAinda não há avaliações
- 2007 Diagnosis and Management of Hypoglycaemia Beyond The Neonatal Period. PCHHDocumento7 páginas2007 Diagnosis and Management of Hypoglycaemia Beyond The Neonatal Period. PCHHChristine ChambersAinda não há avaliações
- 1964 Acute Diarrhoeal Disease in Less Developed Countries. BWHODocumento12 páginas1964 Acute Diarrhoeal Disease in Less Developed Countries. BWHOChristine ChambersAinda não há avaliações
- Pediatrics 2006 Congenital Hypothyroidism GuidelinesDocumento16 páginasPediatrics 2006 Congenital Hypothyroidism GuidelinesRahmah Shah BahaiAinda não há avaliações
- z1974 Laboratory Screening For Congenital Hypothyroidism. LANCETDocumento3 páginasz1974 Laboratory Screening For Congenital Hypothyroidism. LANCETChristine ChambersAinda não há avaliações
- 1949 Relation of Nutrition To Infection in Children. AJPHNHDocumento4 páginas1949 Relation of Nutrition To Infection in Children. AJPHNHChristine ChambersAinda não há avaliações
- 2015 UK National Screening Committee. Topic Newborn Screening For Cystic Fibrosis. BAZIANDocumento33 páginas2015 UK National Screening Committee. Topic Newborn Screening For Cystic Fibrosis. BAZIANChristine ChambersAinda não há avaliações
- CMPA in Children. When To SuspectDocumento28 páginasCMPA in Children. When To SuspectChristine ChambersAinda não há avaliações
- 2006 Introduction To The Newborn Screening Fact Sheets. PEDDocumento11 páginas2006 Introduction To The Newborn Screening Fact Sheets. PEDChristine ChambersAinda não há avaliações
- 2013 Newborn Screening For Inherited Metabolic Disorders. News and Views. JRMSCDocumento11 páginas2013 Newborn Screening For Inherited Metabolic Disorders. News and Views. JRMSCChristine ChambersAinda não há avaliações
- 2006 Newborn Screening. Toward A Uniform Screening Panel and System (Executive Summary) - PEDDocumento15 páginas2006 Newborn Screening. Toward A Uniform Screening Panel and System (Executive Summary) - PEDChristine ChambersAinda não há avaliações
- 2006 Newborn Screening. Toward A Uniform Screening Panel and System (Executive Summary) - PEDDocumento15 páginas2006 Newborn Screening. Toward A Uniform Screening Panel and System (Executive Summary) - PEDChristine ChambersAinda não há avaliações
- 2016 Guidelines For Newborn Blood Spot. NHSDocumento50 páginas2016 Guidelines For Newborn Blood Spot. NHSChristine ChambersAinda não há avaliações
- 2014 Screening Programmes. Newborn Blood Spot. NICEDocumento5 páginas2014 Screening Programmes. Newborn Blood Spot. NICEChristine ChambersAinda não há avaliações
- 2003 Population Genetic Screening Programmes. Principles, Techniques, Practices, and Policies. EJHGDocumento39 páginas2003 Population Genetic Screening Programmes. Principles, Techniques, Practices, and Policies. EJHGChristine ChambersAinda não há avaliações
- 2006 Postnatal Care Up To 8 Weeks After Birth. NICEDocumento63 páginas2006 Postnatal Care Up To 8 Weeks After Birth. NICEChristine ChambersAinda não há avaliações
- 2014 BSACI Guideline For The Diagnosis and Management of Cow's Milk Allergy. CEADocumento31 páginas2014 BSACI Guideline For The Diagnosis and Management of Cow's Milk Allergy. CEAChristine ChambersAinda não há avaliações
- 1998 Inborn Errors of Metabolism in Infancy. A Guide To Diagnosis. PEDDocumento11 páginas1998 Inborn Errors of Metabolism in Infancy. A Guide To Diagnosis. PEDChristine ChambersAinda não há avaliações
- 2016 CDC Guideline For Prescribing Opioids For Chronic Pain US. CDCDocumento52 páginas2016 CDC Guideline For Prescribing Opioids For Chronic Pain US. CDCChristine ChambersAinda não há avaliações
- 2011 Food Allergy in Under 19s. Assessment and Diagnosis. NICEDocumento27 páginas2011 Food Allergy in Under 19s. Assessment and Diagnosis. NICEChristine ChambersAinda não há avaliações
- Evaluation of Transcutaneous Electrical Posterior Tibial Nerve Stimulation For The Treatment of Fecal and Urinary Leaks in Children. JPS 2015Documento4 páginasEvaluation of Transcutaneous Electrical Posterior Tibial Nerve Stimulation For The Treatment of Fecal and Urinary Leaks in Children. JPS 2015Christine ChambersAinda não há avaliações
- 2016 Sepsis-Induced Myocardial Dysfunction. Pathophysiology and Management. JICDocumento10 páginas2016 Sepsis-Induced Myocardial Dysfunction. Pathophysiology and Management. JICChristine Chambers100% (1)
- 2016 Status of Vaccine Research and Development of Vaccines For Tuberculosis. VACCINEDocumento4 páginas2016 Status of Vaccine Research and Development of Vaccines For Tuberculosis. VACCINEChristine ChambersAinda não há avaliações
- 2013 Guideline For Colonoscopy Quality Assurance in Ontario. CCODocumento84 páginas2013 Guideline For Colonoscopy Quality Assurance in Ontario. CCOChristine ChambersAinda não há avaliações
- 2016 Perspectives On Treatment For Nonalcoholic Steatohepatitis. GASTROENTDocumento36 páginas2016 Perspectives On Treatment For Nonalcoholic Steatohepatitis. GASTROENTChristine ChambersAinda não há avaliações
- 2016 Status of Vaccine Research and Development of Vaccines For Tuberculosis. VACCINEDocumento4 páginas2016 Status of Vaccine Research and Development of Vaccines For Tuberculosis. VACCINEChristine ChambersAinda não há avaliações
- Guillian Barre SyndromeDocumento11 páginasGuillian Barre SyndromemohamedAinda não há avaliações
- 2006 Clinical Studies of Pediatric Malabsorption Syndromes. FIZDocumento2 páginas2006 Clinical Studies of Pediatric Malabsorption Syndromes. FIZChristine ChambersAinda não há avaliações
- 2014 The Effect of Virtual Endoscopy Simulator Training On Novices. PLOSONEDocumento9 páginas2014 The Effect of Virtual Endoscopy Simulator Training On Novices. PLOSONEChristine ChambersAinda não há avaliações
- LifeWave X39 Pilot Demuestra Cambios Ligeros ActivadosDocumento12 páginasLifeWave X39 Pilot Demuestra Cambios Ligeros Activadosave_fenix_mileniumAinda não há avaliações
- Protein Structure and FucntionsDocumento59 páginasProtein Structure and FucntionsTiffany Shane VallenteAinda não há avaliações
- Exam 2020Documento34 páginasExam 2020Sameh NoorAinda não há avaliações
- Protein Metabolism and Urea Recycling in Rodent HibernatorsDocumento5 páginasProtein Metabolism and Urea Recycling in Rodent HibernatorsBud Marvin LeRoy RiedeselAinda não há avaliações
- Natural FibresDocumento25 páginasNatural FibresDr.-Ing. Priyadarshini RAinda não há avaliações
- CPP (Biomolecules) : Part - I: Subjective QuestionsDocumento15 páginasCPP (Biomolecules) : Part - I: Subjective QuestionsFalgun SoniAinda não há avaliações
- TGP Alt FluitestDocumento4 páginasTGP Alt FluitestCristian LaraAinda não há avaliações
- 9701 w03 QP 4Documento12 páginas9701 w03 QP 4Hendrawan SaputraAinda não há avaliações
- Amino Acid CatabolismDocumento24 páginasAmino Acid CatabolismAnonymous 0ha8TmAinda não há avaliações
- Original Article Sensory Aroma From Maillard Reaction of Individual and Combinations of Amino Acids With Glucose in Acidic ConditionsDocumento8 páginasOriginal Article Sensory Aroma From Maillard Reaction of Individual and Combinations of Amino Acids With Glucose in Acidic ConditionsBoooooooseAinda não há avaliações
- Endogenous Protoporphyrin IX, A Clinically Useful Photosensitizer For Photodynamic TherapyDocumento18 páginasEndogenous Protoporphyrin IX, A Clinically Useful Photosensitizer For Photodynamic TherapyYerly Ramirez MuñozAinda não há avaliações
- Visit The National Academies Press Online and Register For..Documento186 páginasVisit The National Academies Press Online and Register For..OsamaAliMoussaAinda não há avaliações
- 11-01 Amino Acids - Nitrogen DisposalDocumento53 páginas11-01 Amino Acids - Nitrogen DisposalFrankenstein MelancholyAinda não há avaliações
- CHE 111 Tutorial 2 Semester I 2021Documento4 páginasCHE 111 Tutorial 2 Semester I 2021Pasmore ndelekiAinda não há avaliações
- PROTEIN (Polypeptide) : Protein: Senyawa Organik Yang Merupakan Polimer Asam Amino Penyusun ProteinDocumento79 páginasPROTEIN (Polypeptide) : Protein: Senyawa Organik Yang Merupakan Polimer Asam Amino Penyusun ProteinDwinur ChasanahAinda não há avaliações
- Budi Altgpt - Doc NewDocumento3 páginasBudi Altgpt - Doc NewIrvanda ENVIOUSAinda não há avaliações
- Pared BacteriasDocumento18 páginasPared BacteriasenadesAinda não há avaliações
- Nitrogen MetabolismDocumento75 páginasNitrogen MetabolismAndreas AndreouAinda não há avaliações
- CA0002OCDocumento27 páginasCA0002OCYourChemistryTeacherAinda não há avaliações
- Chem 160.1 Post LabDocumento7 páginasChem 160.1 Post LabMarlyn AmanteAinda não há avaliações
- Ts-1 Production of Flavouring Agent From Shrimp HeadsDocumento8 páginasTs-1 Production of Flavouring Agent From Shrimp HeadsRemya PillaiAinda não há avaliações
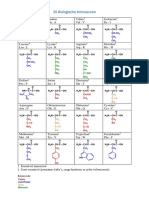
- 20 Biologische Aminozuren: Asparaginezuur Asp DDocumento2 páginas20 Biologische Aminozuren: Asparaginezuur Asp Detienne.jooken8734Ainda não há avaliações
- Kurokawa 1994Documento9 páginasKurokawa 1994Степан РемыгаAinda não há avaliações
- Amino Acids: Associate Professor Ljiljana Andrijević Department of BiochemistryDocumento41 páginasAmino Acids: Associate Professor Ljiljana Andrijević Department of BiochemistryVanja PlavšićAinda não há avaliações
- ALTDocumento10 páginasALTLiviu Athos Tamas0% (1)
- Appendix I Estimation of Acid Phosphatase: PrincipleDocumento39 páginasAppendix I Estimation of Acid Phosphatase: PrincipleSurya PrakashAinda não há avaliações
- Vce Chemistry Data Book Annotated For 2021 v3Documento15 páginasVce Chemistry Data Book Annotated For 2021 v3Mahhe AbdulahiAinda não há avaliações