Você também pode gostar
- UltrasonicDocumento5 páginasUltrasoniclgrome73100% (1)
- 3D Ultrasonic ImagingDocumento5 páginas3D Ultrasonic ImagingriannataAinda não há avaliações
- Timers and InterruptsDocumento75 páginasTimers and InterruptsriannataAinda não há avaliações
- SVMDocumento12 páginasSVMNarmatha BalachandarAinda não há avaliações
- 111061111Documento9 páginas111061111riannataAinda não há avaliações
- 15 4Documento19 páginas15 4SitisaifulAinda não há avaliações
- LV MaxSonar EZ DatasheetDocumento11 páginasLV MaxSonar EZ Datasheetriannata100% (2)
- Space-Frequency AtomsDocumento20 páginasSpace-Frequency AtomsriannataAinda não há avaliações
- Signal Model For The Prediction of Wind Speed in NigeriaDocumento8 páginasSignal Model For The Prediction of Wind Speed in NigeriariannataAinda não há avaliações
- 63-No.4-2008 - 04-Svilainis, MotiejunasDocumento5 páginas63-No.4-2008 - 04-Svilainis, MotiejunasriannataAinda não há avaliações
- Space-Frequency AtomsDocumento20 páginasSpace-Frequency AtomsriannataAinda não há avaliações
- Multipath Cross-Correlation Flowmeters: V. Skwarek and V. HansDocumento6 páginasMultipath Cross-Correlation Flowmeters: V. Skwarek and V. HansriannataAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5783)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Multiple Switch Detection Interface With Suppressed Wake-Up: Technical DataDocumento32 páginasMultiple Switch Detection Interface With Suppressed Wake-Up: Technical Datakatty cumbeAinda não há avaliações
- Ca7050 Lan TesterDocumento3 páginasCa7050 Lan TesterIni AtnAinda não há avaliações
- SW-Update-Guide Powador 6.0-20.0 TL3 V3.31 enDocumento2 páginasSW-Update-Guide Powador 6.0-20.0 TL3 V3.31 enS M NaveedAinda não há avaliações
- DC-DC Part 6 DoubleDocumento18 páginasDC-DC Part 6 DoubleDefne AktemizAinda não há avaliações
- Technical Data: GW4000-DT GW5000-DT GW5000L-DT GW6000-DT GW6000L-DT GW8000-DT GW10KN-DT GW10KL-DTDocumento1 páginaTechnical Data: GW4000-DT GW5000-DT GW5000L-DT GW6000-DT GW6000L-DT GW8000-DT GW10KN-DT GW10KL-DTShimmy AntonyAinda não há avaliações
- Testing of DC MachinesDocumento5 páginasTesting of DC Machines2K20EE102 GauravAinda não há avaliações
- N PN PNP Transistor Lesson 01 ADocumento29 páginasN PN PNP Transistor Lesson 01 ANooruddin SheikAinda não há avaliações
- 06.0 PLC Processor 174 PDFDocumento1 página06.0 PLC Processor 174 PDFSatyasrinivas PulavarthiAinda não há avaliações
- Unipolar To Bipolar Analog Voltage ConversionDocumento20 páginasUnipolar To Bipolar Analog Voltage ConversionGautam MonipatroAinda não há avaliações
- Lm393 Motor Speed Measuring Sensor Module For ArduinoDocumento2 páginasLm393 Motor Speed Measuring Sensor Module For ArduinovivekanandkAinda não há avaliações
- The 8051 Microcontroller and Embedded Systems Using Assembly and C PDFDocumento542 páginasThe 8051 Microcontroller and Embedded Systems Using Assembly and C PDFAli Baig67% (3)
- Lecture 2 Digital Modulation PDFDocumento9 páginasLecture 2 Digital Modulation PDFRokuichi Web ProgrammerAinda não há avaliações
- Tower Ups With Automatic Voltage Regulation: Ut SeriesDocumento2 páginasTower Ups With Automatic Voltage Regulation: Ut SeriesGoogle HomeAinda não há avaliações
- Chapter 3 - Current Electricity Case Study/ Source Based Question 1Documento2 páginasChapter 3 - Current Electricity Case Study/ Source Based Question 1Daksh YadavAinda não há avaliações
- Scan FABDocumento2 páginasScan FABqlx4Ainda não há avaliações
- FT 450DDocumento102 páginasFT 450DSandro TolosaAinda não há avaliações
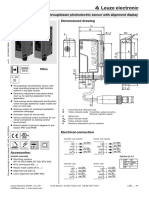
- L46C Red-Light Throughbeam Photoelectric Sensor With Alignment DisplayDocumento4 páginasL46C Red-Light Throughbeam Photoelectric Sensor With Alignment DisplayHaris AhmadAinda não há avaliações
- DP LAN Others 13115 DriversDocumento2.284 páginasDP LAN Others 13115 DriversSyed AliAinda não há avaliações
- EST3Documento4 páginasEST3Juan Dela CruzAinda não há avaliações
- CHF100 English Manual INVT - 1.4.1Documento136 páginasCHF100 English Manual INVT - 1.4.1Mandala DevilDiceAinda não há avaliações
- 4-Analog InputDocumento21 páginas4-Analog InputTam PhamAinda não há avaliações
- UNIT - 1 - AC Characteristics and Frequency ResponceDocumento18 páginasUNIT - 1 - AC Characteristics and Frequency ResponceGauthiAinda não há avaliações
- Multimedia Systems ExplainedDocumento9 páginasMultimedia Systems ExplainedThomas KimAinda não há avaliações
- Micom P547 Phase Comparison ProtectionDocumento2 páginasMicom P547 Phase Comparison Protectiondave chaudhuryAinda não há avaliações
- IC-Applications U4Documento21 páginasIC-Applications U4kavithavenkatesanAinda não há avaliações
- TS GENCO Assistant Engineer Syllabus Previous Papers 2015 Electrical, Mechanical, Civil, Electronics - Recruitment Notification 2015, Govt Jobs 2015Documento3 páginasTS GENCO Assistant Engineer Syllabus Previous Papers 2015 Electrical, Mechanical, Civil, Electronics - Recruitment Notification 2015, Govt Jobs 2015Mir Mustafa Ali50% (2)
- ParadoxDocumento7 páginasParadoxLisa FloresAinda não há avaliações
- Passport 8600 Product BriefDocumento96 páginasPassport 8600 Product BriefKevin Lopo1100% (2)
- Economical 4U Rackmount Chassis with Front USB PS/2Documento2 páginasEconomical 4U Rackmount Chassis with Front USB PS/2Stelvio QuizolaAinda não há avaliações