Você também pode gostar
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingNo EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingAinda não há avaliações
- National Stroke Thrombolysis Guideline Template v9 5-12-13 FINAL 2Documento15 páginasNational Stroke Thrombolysis Guideline Template v9 5-12-13 FINAL 2Muhammad FauziAinda não há avaliações
- Peri - Operative ManagementDocumento32 páginasPeri - Operative Managementrichamalik99Ainda não há avaliações
- Day in The Life 2019Documento30 páginasDay in The Life 2019Hoa Cỏ ĐậuAinda não há avaliações
- Coronary Artery DiseaseDocumento32 páginasCoronary Artery DiseasecjissamAinda não há avaliações
- 2021 ACLS Study GuideDocumento20 páginas2021 ACLS Study GuideShane Brown83% (12)
- Shock ManagementDocumento26 páginasShock ManagementMuhammad Irfanuddin Bin IbrahimAinda não há avaliações
- Traumatic Brain Injury 2023Documento17 páginasTraumatic Brain Injury 2023Fernando Martinez AguilarAinda não há avaliações
- Brain Death Testing Protocol (Rev220605) PDFDocumento2 páginasBrain Death Testing Protocol (Rev220605) PDFRei Irinco100% (1)
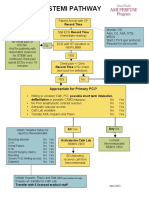
- ME10!03!003 MMC Pathway2Documento2 páginasME10!03!003 MMC Pathway2Indra WijayaAinda não há avaliações
- Afib Protocol Exclusion CriteriaDocumento3 páginasAfib Protocol Exclusion CriteriaJesse M. MassieAinda não há avaliações
- Saudi CPR Guidlines in EnglishDocumento16 páginasSaudi CPR Guidlines in EnglishpiyushbamsAinda não há avaliações
- ACLS Pocket CardDocumento6 páginasACLS Pocket Cardno_spam_mang80% (5)
- Major Haemorrhage ProtocolsDocumento3 páginasMajor Haemorrhage ProtocolsleicesterbugAinda não há avaliações
- Admission To The ICU and Monitoring Technique Early Postoperative CareDocumento7 páginasAdmission To The ICU and Monitoring Technique Early Postoperative CareWidiartha WahyudiAinda não há avaliações
- Medical Scenario 1Documento42 páginasMedical Scenario 1murphy 1087Ainda não há avaliações
- Clinical Pathway StrokeDocumento8 páginasClinical Pathway StrokedjizhieeAinda não há avaliações
- ACLS Simulation ScenariosDocumento14 páginasACLS Simulation ScenariosVanessa HermioneAinda não há avaliações
- Surgical Intern Survival GuideDocumento85 páginasSurgical Intern Survival Guidesgod34100% (1)
- Sepsis Flow Chart FinalDocumento2 páginasSepsis Flow Chart FinalDevindraPrptAinda não há avaliações
- Cerebrovascular Accident Case StudyDocumento5 páginasCerebrovascular Accident Case StudyShainae meriolesAinda não há avaliações
- The Rules and Changes: ACLS Guidelines 2010Documento81 páginasThe Rules and Changes: ACLS Guidelines 2010Annisa Rizki Ratih PratiwiAinda não há avaliações
- An Introduction To Obstetrical Emergencies: Charles D Giordano CRNA, MSNDocumento49 páginasAn Introduction To Obstetrical Emergencies: Charles D Giordano CRNA, MSNEffendi ZakriAinda não há avaliações
- BLS and Advance Cardiac Life SupportDocumento135 páginasBLS and Advance Cardiac Life SupportSteffiAinda não há avaliações
- Icu Cheat Sheet Working FileDocumento7 páginasIcu Cheat Sheet Working FileBhumiShahAinda não há avaliações
- Paediatric Clinical GuidelinesDocumento7 páginasPaediatric Clinical GuidelinesAndriAinda não há avaliações
- Vent ProtocolDocumento15 páginasVent Protocolihtisham1Ainda não há avaliações
- AclsDocumento73 páginasAclsKamel Hady50% (2)
- Anaesthetic Management of PheochromocytomaDocumento22 páginasAnaesthetic Management of PheochromocytomaZoelAinda não há avaliações
- Airway Management 19 IndDocumento29 páginasAirway Management 19 IndChi MutiaAinda não há avaliações
- CCU Clinical GuidelinesDocumento63 páginasCCU Clinical GuidelinesHAMMYER ALROKHAMIAinda não há avaliações
- ACLS NotesDocumento9 páginasACLS Notestasha0% (1)
- Life Support DocumentDocumento9 páginasLife Support DocumentThe Print shopAinda não há avaliações
- Mechanical ThrombectomyDocumento58 páginasMechanical Thrombectomyres.uditacharyaAinda não há avaliações
- Postanesthesia Care: Muhamad Chairul FadhilDocumento28 páginasPostanesthesia Care: Muhamad Chairul FadhilMuhammad Chairul Fadhil100% (1)
- Exchange TransfusionDocumento35 páginasExchange Transfusionsobinjohnpkl100% (2)
- Sample Case ScenarioDocumento8 páginasSample Case ScenarioJan Crizza Dale R. FrancoAinda não há avaliações
- Client Information Sheet (CIS)Documento10 páginasClient Information Sheet (CIS)Christine RombawaAinda não há avaliações
- Guidelines For The Management of Acute Stroke: Emergency DepartmentDocumento10 páginasGuidelines For The Management of Acute Stroke: Emergency DepartmentUhuebor DavidAinda não há avaliações
- Iat Sepsis v7 3Documento1 páginaIat Sepsis v7 3api-296123515Ainda não há avaliações
- Pediatric Life Support SHGDocumento32 páginasPediatric Life Support SHGIwan SinagaAinda não há avaliações
- Hellp Made EasyDocumento52 páginasHellp Made EasyJanuary V. Yabut-DucducanAinda não há avaliações
- EMA ProtocolsDocumento14 páginasEMA ProtocolsMattAinda não há avaliações
- Code Blue ManagemnetDocumento36 páginasCode Blue ManagemnetPreethi BAinda não há avaliações
- SP50 Cardiac Stress-Exercise Testing (Adult, Peds)Documento8 páginasSP50 Cardiac Stress-Exercise Testing (Adult, Peds)Sonu JacobAinda não há avaliações
- MH Guideline For Web v2Documento1 páginaMH Guideline For Web v2FilbertaAinda não há avaliações
- CCS - Handbook of Anesthesiology (2005)Documento180 páginasCCS - Handbook of Anesthesiology (2005)Rojelle LezamaAinda não há avaliações
- O&G Off-Tag Assesment Logbook: Traces-Pdf-248732173Documento9 páginasO&G Off-Tag Assesment Logbook: Traces-Pdf-248732173niwasAinda não há avaliações
- TPA Protocol: Stroke in Carefully Selected PersonsDocumento4 páginasTPA Protocol: Stroke in Carefully Selected PersonsJavier Gonzalez, M.D. DABEMAinda não há avaliações
- Advanced Cardiac Life SupportDocumento42 páginasAdvanced Cardiac Life SupportDennis MiritiAinda não há avaliações
- R1 Orientation, Oncall Issues.Documento55 páginasR1 Orientation, Oncall Issues.latifaAinda não há avaliações
- Update in Stroke Management: David Lee Gordon, M.D., FAHADocumento43 páginasUpdate in Stroke Management: David Lee Gordon, M.D., FAHAMuhidin AeAinda não há avaliações
- Assessment of The Acutely Ill PatientDocumento10 páginasAssessment of The Acutely Ill PatientZacmilo Dela TorreAinda não há avaliações
- 4 Weaning Ventilator-NIADocumento31 páginas4 Weaning Ventilator-NIAResyana Widyayani100% (1)
- Advanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesNo EverandAdvanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesNota: 4 de 5 estrelas4/5 (6)
- Hpwriteup OutlineDocumento5 páginasHpwriteup OutlinemsmodcAinda não há avaliações
- Intern History SheetDocumento2 páginasIntern History SheetmaddythedocAinda não há avaliações
- Mechanical VentilationDocumento11 páginasMechanical VentilationmaddythedocAinda não há avaliações
- Mechanical VentilationDocumento11 páginasMechanical VentilationmaddythedocAinda não há avaliações
- An Approach To The Evaluation of A Patient For Seizures and EpilepsyDocumento8 páginasAn Approach To The Evaluation of A Patient For Seizures and EpilepsyGaneshRajaratenamAinda não há avaliações
- PalsDocumento12 páginasPalsGhadeer EbraheemAinda não há avaliações
- Pediatrics Milestones ChartDocumento32 páginasPediatrics Milestones ChartmaddythedocAinda não há avaliações
- History Taking ExaminationDocumento7 páginasHistory Taking ExaminationIndunil AnuruddhikaAinda não há avaliações
- MIT Medical Department Pediatrics History Form: AppointmentDocumento4 páginasMIT Medical Department Pediatrics History Form: Appointmentmaddythedoc100% (1)
- Outline of Physical ExaminationDocumento10 páginasOutline of Physical ExaminationmaddythedocAinda não há avaliações
- FrostbiteDocumento1 páginaFrostbitemaddythedocAinda não há avaliações
- Stroke AlgoDocumento59 páginasStroke AlgomaddythedocAinda não há avaliações
- UPenn Clinic GuideDocumento114 páginasUPenn Clinic GuideVeronica AlexanderAinda não há avaliações
- Differential List (No. To Revise) : H. Weakness/ NumbnessDocumento3 páginasDifferential List (No. To Revise) : H. Weakness/ NumbnessmaddythedocAinda não há avaliações
- WHO AM I - Casting CrownsDocumento1 páginaWHO AM I - Casting CrownsMarcos otoniAinda não há avaliações
- Gaslands - Refuelled - Overdrive - No 4 - EN (OEF) (2021!12!25)Documento20 páginasGaslands - Refuelled - Overdrive - No 4 - EN (OEF) (2021!12!25)nispotulmi100% (1)
- Beaufort Wind Scale, Weather, Ice, Tides y Ship Motions EquipmentDocumento5 páginasBeaufort Wind Scale, Weather, Ice, Tides y Ship Motions EquipmentAndres Garcia VisbalAinda não há avaliações
- Question: "The Himalayas Are Highly Prone To Landslides. "Discuss The Causes and Suggest Suitable Measures of Mitigation. SolutionDocumento3 páginasQuestion: "The Himalayas Are Highly Prone To Landslides. "Discuss The Causes and Suggest Suitable Measures of Mitigation. SolutionMukund Anand 16BIT0287Ainda não há avaliações
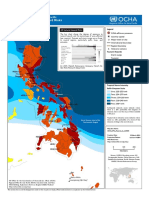
- Phil Natural Hazard Map PDFDocumento1 páginaPhil Natural Hazard Map PDFmarcamilleAinda não há avaliações
- Components of DamsDocumento37 páginasComponents of DamsAmanuel AzemeteAinda não há avaliações
- ITC Corporate Strategy AnalysisDocumento46 páginasITC Corporate Strategy Analysisstanleyjebakumar2Ainda não há avaliações
- 10th ChemistryDocumento4 páginas10th ChemistrySana AshfaqAinda não há avaliações
- ABB ESE Technology Explanation Rev1Documento45 páginasABB ESE Technology Explanation Rev1vikivarma147Ainda não há avaliações
- GE1.7 Technical DescriptionDocumento10 páginasGE1.7 Technical DescriptionChristopher SchoberAinda não há avaliações
- A Detailed Lesson Plan in Science 8Documento11 páginasA Detailed Lesson Plan in Science 8Isabelo De Asis Alferez100% (1)
- Taran - Sgi La BrochureDocumento2 páginasTaran - Sgi La Brochurechaman kumarAinda não há avaliações
- Tools For High Performance Building Designers: ASHRAE's HVAC Design: Level I Essentials (MENA)Documento2 páginasTools For High Performance Building Designers: ASHRAE's HVAC Design: Level I Essentials (MENA)Lisma RantoAinda não há avaliações
- Pilot's Handbook of Aeronautical Knowledge ADocumento471 páginasPilot's Handbook of Aeronautical Knowledge AJustin100% (4)
- Assam (Geography)Documento11 páginasAssam (Geography)Shristi KrishnaAinda não há avaliações
- Thunder and LightningDocumento6 páginasThunder and Lightningapi-198617400Ainda não há avaliações
- Hurricane Zeta ReportDocumento56 páginasHurricane Zeta ReportThe Courier and Daily CometAinda não há avaliações
- QUARTER 3 Summative Test G9Documento6 páginasQUARTER 3 Summative Test G9Angelita MenesesAinda não há avaliações
- Wind Speed Gust DurationDocumento12 páginasWind Speed Gust DurationHomer SilvaAinda não há avaliações
- Climate of Leh: Winter SnowfallDocumento5 páginasClimate of Leh: Winter SnowfallYashlokDuttAinda não há avaliações
- Ultrasonic Anemometer 3DDocumento4 páginasUltrasonic Anemometer 3DmitziAinda não há avaliações
- TBS Earthing SystemsDocumento81 páginasTBS Earthing SystemsJanko GardaševićAinda não há avaliações
- Barograph - Wikipedia, The Free Encyclopedia PDFDocumento3 páginasBarograph - Wikipedia, The Free Encyclopedia PDFelvi anggiovennyAinda não há avaliações
- Vijayavenkataraman2012 PDFDocumento20 páginasVijayavenkataraman2012 PDFAhmad Jawid StanikzaiAinda não há avaliações
- 124 Map Pointing Skills Guidelines For Class X 20190906165519Documento2 páginas124 Map Pointing Skills Guidelines For Class X 20190906165519HARRY POTTERAinda não há avaliações
- Adfdp182 6565B XDMDocumento3 páginasAdfdp182 6565B XDMmapat99Ainda não há avaliações
- MeteorologyDocumento52 páginasMeteorologyRodel Rosales100% (1)
- Xihoumen BridgeDocumento14 páginasXihoumen Bridgejygfrit100% (1)
- Tornadogenesis Presentation - Markowski - InGDocumento29 páginasTornadogenesis Presentation - Markowski - InGDellmannsAinda não há avaliações
- Ambient Weather WS-2080 Wireless Home Weather StationDocumento41 páginasAmbient Weather WS-2080 Wireless Home Weather StationJohn G.Ainda não há avaliações