Você também pode gostar
- Health Literacy: Concept Analysis: Carolyn SperosDocumento8 páginasHealth Literacy: Concept Analysis: Carolyn Speroscheurl mizanAinda não há avaliações
- ED508707Documento41 páginasED508707Ronnel VelascoAinda não há avaliações
- Improving Doctor-Patient Communication for Those With Low Health LiteracyDocumento7 páginasImproving Doctor-Patient Communication for Those With Low Health LiteracymeyfitaAinda não há avaliações
- Journal of Information Literacy: ISSN 1750-5968Documento15 páginasJournal of Information Literacy: ISSN 1750-5968hairun hairunAinda não há avaliações
- Health Literacy Among Older Adults A Systematic Literature ReviewDocumento4 páginasHealth Literacy Among Older Adults A Systematic Literature ReviewcmaqqsrifAinda não há avaliações
- Ananotaed BibliographyDocumento12 páginasAnanotaed BibliographyElvis Rodgers DenisAinda não há avaliações
- Health Literacy and Public Health: A Systematic Review and Integration of Definitions and ModelsDocumento13 páginasHealth Literacy and Public Health: A Systematic Review and Integration of Definitions and ModelsAnis RanisAinda não há avaliações
- 8007-Article Text-31924-1-10-20130814Documento6 páginas8007-Article Text-31924-1-10-20130814josephAinda não há avaliações
- Social Science & Medicine: Sian K. Smith, Ann Dixon, Lyndal Trevena, Don Nutbeam, Kirsten J. MccafferyDocumento8 páginasSocial Science & Medicine: Sian K. Smith, Ann Dixon, Lyndal Trevena, Don Nutbeam, Kirsten J. MccafferySteven WoodheadAinda não há avaliações
- Importance of cultural competency and health literacyDocumento4 páginasImportance of cultural competency and health literacycollins hagembeAinda não há avaliações
- Preventative Healthcare Literature ReviewDocumento8 páginasPreventative Healthcare Literature Reviewapi-290166100100% (1)
- Young Adults' Health Perceptions, Behaviors and Info SeekingDocumento19 páginasYoung Adults' Health Perceptions, Behaviors and Info SeekingKITTIVONGSAK VONGSUTHEP KEITHAinda não há avaliações
- Chapter 2 Reviewsof Related Literatureand Related Studies TopicalDocumento14 páginasChapter 2 Reviewsof Related Literatureand Related Studies Topicalr76914751Ainda não há avaliações
- A Review of Literature On Access To Primary Health CareDocumento5 páginasA Review of Literature On Access To Primary Health CareafmzsbzbczhtbdAinda não há avaliações
- Health Literacy: What Is It?: Journal of Health CommunicationDocumento12 páginasHealth Literacy: What Is It?: Journal of Health CommunicationIrnayanti MamiDgSiameAinda não há avaliações
- Low Health Literacy Overview Assesses Steps Toward High-Quality Diabetes CareDocumento8 páginasLow Health Literacy Overview Assesses Steps Toward High-Quality Diabetes CareGONDHES CHANNELAinda não há avaliações
- Ill-Health and Poverty A Literature Review On Health in Informal SettlementsDocumento10 páginasIll-Health and Poverty A Literature Review On Health in Informal Settlementsc5m07hh9Ainda não há avaliações
- Culture, Language, and The Doctor-Patient Relationship: Escholarship@UmmsDocumento10 páginasCulture, Language, and The Doctor-Patient Relationship: Escholarship@UmmsBUAHIN JANNAAinda não há avaliações
- HHS Public Access: Nurse Communication Challenges With Health Literacy SupportDocumento17 páginasHHS Public Access: Nurse Communication Challenges With Health Literacy SupportRatih puspita DewiAinda não há avaliações
- Culture Language and The Doctor Patient Relation Ship PDFDocumento10 páginasCulture Language and The Doctor Patient Relation Ship PDFWagiono SuparanAinda não há avaliações
- The Question of Competence: Reconsidering Medical Education in the Twenty-First CenturyNo EverandThe Question of Competence: Reconsidering Medical Education in the Twenty-First CenturyAinda não há avaliações
- Handbook of Life Course Health DevelopmentDocumento667 páginasHandbook of Life Course Health DevelopmentCait KantorAinda não há avaliações
- Mental Health and Palliative Care Literature ReviewDocumento4 páginasMental Health and Palliative Care Literature ReviewafdtbwkhbAinda não há avaliações
- Distributed Health Literacy in The Maternal Health Context in VietnamDocumento12 páginasDistributed Health Literacy in The Maternal Health Context in Vietnamhairun hairunAinda não há avaliações
- Nutrition and Health Literacy A Systematic ReviewDocumento13 páginasNutrition and Health Literacy A Systematic ReviewJanelle Louise BarreraAinda não há avaliações
- Health Literacy: Essential For A Culture of HealthDocumento7 páginasHealth Literacy: Essential For A Culture of HealthasriadiAinda não há avaliações
- A Systematic Review of The Literature On Health Literacy in Nursing EducationDocumento5 páginasA Systematic Review of The Literature On Health Literacy in Nursing EducationKusrini Kadar SyamsalamAinda não há avaliações
- Why People Use Health Services by Irwin M. RosenstockDocumento32 páginasWhy People Use Health Services by Irwin M. RosenstockBuyTheBidAinda não há avaliações
- The Health Care Handbook - A Clear and Concise Guide To The United States Health Care System, 2nd EditionDocumento321 páginasThe Health Care Handbook - A Clear and Concise Guide To The United States Health Care System, 2nd EditionSOUFIANE RACHID78% (9)
- Educating Nursing Students About Health Literacy - From The Classroom To The Patient BedsideDocumento11 páginasEducating Nursing Students About Health Literacy - From The Classroom To The Patient BedsideKusrini Kadar SyamsalamAinda não há avaliações
- Health LiteracyDocumento5 páginasHealth LiteracyHillary JamesAinda não há avaliações
- Samerski-Health Literacy As A Social Practice - Pdf-OptionalDocumento8 páginasSamerski-Health Literacy As A Social Practice - Pdf-OptionalSarah El HalabiAinda não há avaliações
- Science and Morality in Medicine: A Survey of Medical EducatorsNo EverandScience and Morality in Medicine: A Survey of Medical EducatorsAinda não há avaliações
- Paper JICDocumento28 páginasPaper JICHeber LopezAinda não há avaliações
- Article One Review (Deaf People)Documento3 páginasArticle One Review (Deaf People)TimquannaAinda não há avaliações
- How To Write A Public Health Research PaperDocumento8 páginasHow To Write A Public Health Research Paperwqbdxbvkg100% (1)
- Genuis - Constructing 'Sense'Documento15 páginasGenuis - Constructing 'Sense'Maria Elisa Valentim Pickler NicolinoAinda não há avaliações
- Understanding Population Health Terminology: University of WisconsinDocumento24 páginasUnderstanding Population Health Terminology: University of WisconsinKizer Roselynn JamiAinda não há avaliações
- Health Literacy: Implications For Pharmacy Practice: Learning ObjectivesDocumento18 páginasHealth Literacy: Implications For Pharmacy Practice: Learning ObjectivesMajed Mubarak Shannan AlzahraniAinda não há avaliações
- Health Literacy On Hypertension and Functional Health Status Among Elderly of Malabon City, PhilippinesDocumento20 páginasHealth Literacy On Hypertension and Functional Health Status Among Elderly of Malabon City, PhilippinesGlobal Research and Development ServicesAinda não há avaliações
- Health Promot. Int.-2009-Peerson-285-96 PDFDocumento12 páginasHealth Promot. Int.-2009-Peerson-285-96 PDFPooja KapoorAinda não há avaliações
- Literature Review Obesity ResearchDocumento5 páginasLiterature Review Obesity Researchtxklbzukg100% (1)
- Sexual Health: A Literature Review On The Sexual Health Needs of People With Intellectual DisabilitiesDocumento22 páginasSexual Health: A Literature Review On The Sexual Health Needs of People With Intellectual Disabilitiesgirly772346Ainda não há avaliações
- Jurnal 1Documento3 páginasJurnal 1nurul fatmaida purwitasariAinda não há avaliações
- Thesis Proposal HealthliteracyDocumento27 páginasThesis Proposal HealthliteracyChristine Rodriguez-GuerreroAinda não há avaliações
- Recent Developments in Public Health Nursing in The AmericasDocumento23 páginasRecent Developments in Public Health Nursing in The AmericasDevi Boru Panggoaran SitinjakAinda não há avaliações
- Jurnal KedokteranDocumento18 páginasJurnal KedokteranelvandryAinda não há avaliações
- Nursing ResearchDocumento15 páginasNursing Researchsubhashreepal13Ainda não há avaliações
- 03 Reeve-Bell-2008-children-healthy-unhealthy-IJSE-final-manuscriptDocumento37 páginas03 Reeve-Bell-2008-children-healthy-unhealthy-IJSE-final-manuscriptLEANDRO ARAVENAAinda não há avaliações
- Trast Psiq en Niños en El MundoDocumento12 páginasTrast Psiq en Niños en El Mundogustavo blancoAinda não há avaliações
- Chapters 1 To 2. Incomplete. Please Double CheckDocumento19 páginasChapters 1 To 2. Incomplete. Please Double CheckajdgafjsdgaAinda não há avaliações
- Research Paper Public HealthDocumento4 páginasResearch Paper Public Healthzqbyvtukg100% (1)
- Issues in Comtemporary NursingDocumento6 páginasIssues in Comtemporary Nursingapi-684731543Ainda não há avaliações
- Understanding and Applying Medical Anthr (Pages 333-335) (2023!12!13)Documento4 páginasUnderstanding and Applying Medical Anthr (Pages 333-335) (2023!12!13)Rachel SawhAinda não há avaliações
- Public Health Research PapersDocumento7 páginasPublic Health Research Papersp1zajywigyd2100% (1)
- Thesis Health CareDocumento8 páginasThesis Health Careaflpbpcnhjpwkd100% (1)
- Annotated BibliographyDocumento6 páginasAnnotated BibliographyFrancisAinda não há avaliações
- Primary Health Care Literature ReviewDocumento4 páginasPrimary Health Care Literature Reviewafdtbluwq100% (1)
- HCAD 620 Week 3's DiscussionDocumento3 páginasHCAD 620 Week 3's Discussionkelvin oumaAinda não há avaliações
- American Sign Language Interpreters Perceptions of Barriers To Healthcare Communication in Deaf and Hard of Hearing PatientsDocumento6 páginasAmerican Sign Language Interpreters Perceptions of Barriers To Healthcare Communication in Deaf and Hard of Hearing Patientsapi-671390452Ainda não há avaliações
- Dok Baru 2020-02-17 10.38.06Documento2 páginasDok Baru 2020-02-17 10.38.06Septyadi David Eka AryunggaAinda não há avaliações
- Virtual Biology Laboratory (Vlab-Bio) : Scenario-Based Learning ApproachDocumento7 páginasVirtual Biology Laboratory (Vlab-Bio) : Scenario-Based Learning ApproachSeptyadi David Eka AryunggaAinda não há avaliações
- Tanpaper tcm18-41069Documento18 páginasTanpaper tcm18-41069Septyadi David Eka AryunggaAinda não há avaliações
- SELEKSI ADMINISTRASI REKRUTMEN PT. ANGKASA PURA IDocumento26 páginasSELEKSI ADMINISTRASI REKRUTMEN PT. ANGKASA PURA Ijohan170189Ainda não há avaliações
- Call For Nominations API Natural SciencesDocumento2 páginasCall For Nominations API Natural SciencesSeptyadi David Eka AryunggaAinda não há avaliações
- A Guide For Novice Researchers - Design and Development Research MethodsDocumento12 páginasA Guide For Novice Researchers - Design and Development Research MethodsAliff NawiAinda não há avaliações
- Development of Two-Tier Diagnostic Instrument and Assess Students' Understanding in ChemistryDocumento6 páginasDevelopment of Two-Tier Diagnostic Instrument and Assess Students' Understanding in ChemistrySeptyadi David Eka AryunggaAinda não há avaliações
- Frayer ModelDocumento3 páginasFrayer ModelSeptyadi David Eka AryunggaAinda não há avaliações
- 47-1 SambrookDocumento11 páginas47-1 SambrookSeptyadi David Eka AryunggaAinda não há avaliações
- 47-1 SambrookDocumento11 páginas47-1 SambrookSeptyadi David Eka AryunggaAinda não há avaliações
- Cognitive ConflictDocumento19 páginasCognitive ConflictSeptyadi David Eka AryunggaAinda não há avaliações
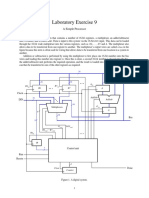
- Laboratory Exercise 9: A Simple ProcessorDocumento8 páginasLaboratory Exercise 9: A Simple ProcessorhxchAinda não há avaliações
- Power: Definition and TypesDocumento3 páginasPower: Definition and TypesShashi RanjanAinda não há avaliações
- CSR FinalDocumento44 páginasCSR FinalrohanAinda não há avaliações
- 320Documento139 páginas320Ashish SharmaAinda não há avaliações
- MeasurIT Flexim WaveInjector 1003Documento3 páginasMeasurIT Flexim WaveInjector 1003cwiejkowskaAinda não há avaliações
- 4024 w13 QP 11 PDFDocumento20 páginas4024 w13 QP 11 PDFChristine SetiawanAinda não há avaliações
- El 114 The-Adventures-of-Tom-Sawyer-by-Mark-TwainDocumento11 páginasEl 114 The-Adventures-of-Tom-Sawyer-by-Mark-TwainGhreniel V. Benecito100% (1)
- Setting TrolleyDocumento19 páginasSetting TrolleyLennard SegundoAinda não há avaliações
- End Term Question Paper - Rural Marketing - Term V Batch 2020-22Documento4 páginasEnd Term Question Paper - Rural Marketing - Term V Batch 2020-22sumit rajAinda não há avaliações
- Default Password For All TMNet Streamyx Supported ModemDocumento2 páginasDefault Password For All TMNet Streamyx Supported ModemFrankly F. ChiaAinda não há avaliações
- Mohammad Akib Nawaz - Scharffen BergerDocumento2 páginasMohammad Akib Nawaz - Scharffen BergerShatakkshi SinghAinda não há avaliações
- AirOS 3.4 - Ubiquiti Wiki#BasicWirelessSettings#BasicWirelessSettingsDocumento24 páginasAirOS 3.4 - Ubiquiti Wiki#BasicWirelessSettings#BasicWirelessSettingsAusAinda não há avaliações
- Scrap Reduction Improvement: Roop Polymers LimitedDocumento5 páginasScrap Reduction Improvement: Roop Polymers Limitedmani01kandanAinda não há avaliações
- Relative ClausesDocumento7 páginasRelative ClausesEvaluna MoidalAinda não há avaliações
- MoRTH CompleteDocumento725 páginasMoRTH CompleteSekharmantri Sitapati85% (71)
- Nuclear Power Corporation of India LimitedDocumento11 páginasNuclear Power Corporation of India Limitedkevin desaiAinda não há avaliações
- LSE100 Past Year Questions (2014/5)Documento2 páginasLSE100 Past Year Questions (2014/5)Jingwen ZhangAinda não há avaliações
- Transactional AnalysisDocumento30 páginasTransactional AnalysissabyasachiAinda não há avaliações
- Mrs Jenny obstetric historyDocumento3 páginasMrs Jenny obstetric historyDwi AnggoroAinda não há avaliações
- Database Design Term Project 1Documento3 páginasDatabase Design Term Project 1MuskanAinda não há avaliações
- 1000 Plus Psychiatry MCQ Book DranilkakunjeDocumento141 páginas1000 Plus Psychiatry MCQ Book Dranilkakunjethelegend 20220% (1)
- State of The Bible 2014 (Barna)Documento65 páginasState of The Bible 2014 (Barna)WolfAinda não há avaliações
- Age of Unreason and Modernity's ContradictionsDocumento4 páginasAge of Unreason and Modernity's ContradictionsKhaled Aryan ArmanAinda não há avaliações
- Emergency procedures for shipboard fire suppression systemsDocumento1 páginaEmergency procedures for shipboard fire suppression systemsImmorthalAinda não há avaliações
- Vanguardia's Online Review Program: Genito-Urinary Tract FunctionDocumento8 páginasVanguardia's Online Review Program: Genito-Urinary Tract FunctionBobet ReñaAinda não há avaliações
- Genetic AlgorithmsDocumento63 páginasGenetic AlgorithmsMuruganandham Subramanian100% (3)
- AP School Education Rules SummaryDocumento17 páginasAP School Education Rules SummaryThirupathaiahAinda não há avaliações
- Laboratory Consumables Price ListDocumento570 páginasLaboratory Consumables Price ListANNISA RAHMATINAAinda não há avaliações
- S.Y. Resistance of A Galvanometer G by Shunting GR - IIDocumento2 páginasS.Y. Resistance of A Galvanometer G by Shunting GR - IINeelam KapoorAinda não há avaliações
- Engineering Economics - Solution Manual (Chapter 1)Documento1 páginaEngineering Economics - Solution Manual (Chapter 1)Diego GuineaAinda não há avaliações