Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Practical Guide Clinical AuditDocumento86 páginasPractical Guide Clinical AuditjhonronAinda não há avaliações
- EMS CatalogDocumento25 páginasEMS Catalogrrockel100% (1)
- Goldman-Cecil Medicine 25th 2015Documento39 páginasGoldman-Cecil Medicine 25th 2015Dumitru HarsenieAinda não há avaliações
- Radiology in UrologyDocumento39 páginasRadiology in UrologyUgan SinghAinda não há avaliações
- Short Bowel SyndromeDocumento50 páginasShort Bowel SyndromeAbdul QadirAinda não há avaliações
- Health Cloud DatasheetDocumento2 páginasHealth Cloud DatasheetMadhuri MalayathiAinda não há avaliações
- Nursing Leadership and ManagementDocumento13 páginasNursing Leadership and ManagementKhatlene Joy RaymundoAinda não há avaliações
- Seronegative Antiphospholipid SyndromeDocumento3 páginasSeronegative Antiphospholipid SyndromealexandruAinda não há avaliações
- BALNEOCLIMATOLOGIEDocumento25 páginasBALNEOCLIMATOLOGIEalexandruAinda não há avaliações
- IASP TaxonomyDocumento8 páginasIASP TaxonomyalexandruAinda não há avaliações
- Assessment of Pain Part - II-Details+DescriptionsDocumento2 páginasAssessment of Pain Part - II-Details+DescriptionsalexandruAinda não há avaliações
- Pain Terms: A Current List With Definitions and Notes On UsageDocumento9 páginasPain Terms: A Current List With Definitions and Notes On UsagealexandruAinda não há avaliações
- Assessment of Pain Part - I-HDocumento1 páginaAssessment of Pain Part - I-HalexandruAinda não há avaliações
- Assessment of Pain Part - II-CDocumento1 páginaAssessment of Pain Part - II-CalexandruAinda não há avaliações
- Assessment of Pain Part - I-DDocumento6 páginasAssessment of Pain Part - I-DalexandruAinda não há avaliações
- Assessment of Pain Part - I-GDocumento7 páginasAssessment of Pain Part - I-GalexandruAinda não há avaliações
- Assessment of Pain PART - I-CDocumento8 páginasAssessment of Pain PART - I-CalexandruAinda não há avaliações
- Assessment of Pain PART - I-ADocumento2 páginasAssessment of Pain PART - I-AalexandruAinda não há avaliações
- GAT NCP Surgery WardDocumento4 páginasGAT NCP Surgery WardDon Richard0% (1)
- Vitamin B Deficiency in Children With Infantile Spasms: A Case-Control StudyDocumento5 páginasVitamin B Deficiency in Children With Infantile Spasms: A Case-Control StudyireneaureliaAinda não há avaliações
- Beer Potomania BrochureDocumento2 páginasBeer Potomania Brochureapi-301611629Ainda não há avaliações
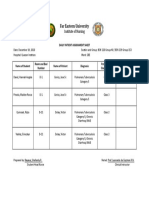
- Daily Patient Assignment SheetDocumento1 páginaDaily Patient Assignment SheetSheferely BayauaAinda não há avaliações
- 12 Shikha Dorgra DentalDocumento4 páginas12 Shikha Dorgra DentalHarish ChowdaryAinda não há avaliações
- American Society For Reproductive MedicineDocumento3 páginasAmerican Society For Reproductive MedicineShanti Natalia NababanAinda não há avaliações
- DPRG FallNewsletter2013Documento8 páginasDPRG FallNewsletter2013RichieDaisyAinda não há avaliações
- Hospital IIIDocumento289 páginasHospital IIIAnu GupteAinda não há avaliações
- Developmental Dysplasia of The Hip: Dr. Bassel El-Osta SPR Trauma & OrthopaedicsDocumento71 páginasDevelopmental Dysplasia of The Hip: Dr. Bassel El-Osta SPR Trauma & OrthopaedicsvadimmadanAinda não há avaliações
- Stab WoundsDocumento15 páginasStab WoundspreveennaAinda não há avaliações
- Easing The Transition From Students To NursesDocumento22 páginasEasing The Transition From Students To Nursesjohn michael olivares67% (3)
- MS Wrep IIDocumento51 páginasMS Wrep IIiana-almocera-6970Ainda não há avaliações
- Actelion Company PresentationDocumento135 páginasActelion Company Presentationmedtechy100% (1)
- Leading Dentist in Oshawa - Scarborough - Grandview Dental ClinicDocumento7 páginasLeading Dentist in Oshawa - Scarborough - Grandview Dental Clinicnaveen bansalAinda não há avaliações
- Diadynamic CurrentDocumento30 páginasDiadynamic Currentpartizan_bl100% (2)
- Operating LightDocumento8 páginasOperating LightrelinAinda não há avaliações
- HRUK Pulse SpringSummer 2013 ScreenDocumento36 páginasHRUK Pulse SpringSummer 2013 ScreenhrukcommunicationsAinda não há avaliações
- Medical Tourism IndiaDocumento3 páginasMedical Tourism IndiafriendsofindiaAinda não há avaliações
- Viral HepatitisDocumento26 páginasViral HepatitisNasriah MacadatoAinda não há avaliações
- Miliue Therapy Skill PDFDocumento1 páginaMiliue Therapy Skill PDFRosalinda SalvadorAinda não há avaliações
- BM Narrative Report - Medical Services IncDocumento35 páginasBM Narrative Report - Medical Services Incjvb_buena2734Ainda não há avaliações
- PisaDocumento2 páginasPisaMrMoezesAinda não há avaliações
- Resume Final 1Documento2 páginasResume Final 1api-308019422Ainda não há avaliações