Você também pode gostar
- 1471-2474-13-81 KonsulDocumento7 páginas1471-2474-13-81 KonsulGustan AriadiAinda não há avaliações
- Emergency Training, Education and Perceived Clinical Skills For Tsunami Care Among Nurses in Banda Aceh, IndonesiaDocumento12 páginasEmergency Training, Education and Perceived Clinical Skills For Tsunami Care Among Nurses in Banda Aceh, IndonesiaGustan AriadiAinda não há avaliações
- Implementation of Recommended Trauma System Criteria in South-Eastern Norway A Cross Sectional Hospital SurveyDocumento7 páginasImplementation of Recommended Trauma System Criteria in South-Eastern Norway A Cross Sectional Hospital SurveyGustan AriadiAinda não há avaliações
- Implementation of Recommended Trauma System Criteria in South-Eastern Norway A Cross Sectional Hospital SurveyDocumento7 páginasImplementation of Recommended Trauma System Criteria in South-Eastern Norway A Cross Sectional Hospital SurveyGustan AriadiAinda não há avaliações
- Emergency Training, Education and Perceived Clinical Skills For Tsunami Care Among Nurses in Banda Aceh, IndonesiaDocumento12 páginasEmergency Training, Education and Perceived Clinical Skills For Tsunami Care Among Nurses in Banda Aceh, IndonesiaGustan AriadiAinda não há avaliações
- WJG 19 7129Documento10 páginasWJG 19 7129Gustan AriadiAinda não há avaliações
- Effect of Educational Outreach To Nurses On Tuberculosis Case Detection and Primary Care of Respiratory Illness Pragmatic ClustDocumento5 páginasEffect of Educational Outreach To Nurses On Tuberculosis Case Detection and Primary Care of Respiratory Illness Pragmatic ClustGustan AriadiAinda não há avaliações
- The Lateral Trauma PositionDocumento5 páginasThe Lateral Trauma PositionGustan AriadiAinda não há avaliações
- Emergency Training, Education and Perceived Clinical Skills For Tsunami Care Among Nurses in Banda Aceh, IndonesiaDocumento12 páginasEmergency Training, Education and Perceived Clinical Skills For Tsunami Care Among Nurses in Banda Aceh, IndonesiaGustan AriadiAinda não há avaliações
- Emergency Training, Education and Perceived Clinical Skills For Tsunami Care Among Nurses in Banda Aceh, IndonesiaDocumento12 páginasEmergency Training, Education and Perceived Clinical Skills For Tsunami Care Among Nurses in Banda Aceh, IndonesiaGustan AriadiAinda não há avaliações
- Implementation of Recommended Trauma System Criteria in South-Eastern Norway A Cross Sectional Hospital SurveyDocumento7 páginasImplementation of Recommended Trauma System Criteria in South-Eastern Norway A Cross Sectional Hospital SurveyGustan AriadiAinda não há avaliações
- Implementation of Recommended Trauma System Criteria in South-Eastern Norway A Cross Sectional Hospital SurveyDocumento7 páginasImplementation of Recommended Trauma System Criteria in South-Eastern Norway A Cross Sectional Hospital SurveyGustan AriadiAinda não há avaliações
- Clinical Review - Initial Management of Blunt Pelvic Trauma Patients With Haemodynamic InstabilityDocumento9 páginasClinical Review - Initial Management of Blunt Pelvic Trauma Patients With Haemodynamic InstabilityGustan AriadiAinda não há avaliações
- Teaching Basic Life Support Algorithms by Either Multimedia Presentations or Case Based Discussion Equally Improves The Level oDocumento8 páginasTeaching Basic Life Support Algorithms by Either Multimedia Presentations or Case Based Discussion Equally Improves The Level oGustan AriadiAinda não há avaliações
- Implementation of Recommended Trauma System Criteria in South-Eastern Norway A Cross Sectional Hospital SurveyDocumento7 páginasImplementation of Recommended Trauma System Criteria in South-Eastern Norway A Cross Sectional Hospital SurveyGustan AriadiAinda não há avaliações
- Effect of Educational Outreach To Nurses On Tuberculosis Case Detection and Primary Care of Respiratory Illness Pragmatic ClustDocumento5 páginasEffect of Educational Outreach To Nurses On Tuberculosis Case Detection and Primary Care of Respiratory Illness Pragmatic ClustGustan AriadiAinda não há avaliações
- Effect of Educational Outreach To Nurses On Tuberculosis Case Detection and Primary Care of Respiratory Illness Pragmatic ClustDocumento5 páginasEffect of Educational Outreach To Nurses On Tuberculosis Case Detection and Primary Care of Respiratory Illness Pragmatic ClustGustan AriadiAinda não há avaliações
- Clinical Outcomes of Patients Requiring Ventilatory Support in Brazilian Intensive Care Units - A Multicenter, Prospective, Cohor-2Documento39 páginasClinical Outcomes of Patients Requiring Ventilatory Support in Brazilian Intensive Care Units - A Multicenter, Prospective, Cohor-2Gustan AriadiAinda não há avaliações
- Emergency Training, Education and Perceived Clinical Skills For Tsunami Care Among Nurses in Banda Aceh, IndonesiaDocumento12 páginasEmergency Training, Education and Perceived Clinical Skills For Tsunami Care Among Nurses in Banda Aceh, IndonesiaGustan AriadiAinda não há avaliações
- Clinical Outcomes of Patients Requiring Ventilatory Support in Brazilian Intensive Care Units - A Multicenter, Prospective, Cohor-2Documento39 páginasClinical Outcomes of Patients Requiring Ventilatory Support in Brazilian Intensive Care Units - A Multicenter, Prospective, Cohor-2Gustan AriadiAinda não há avaliações
- Qual Saf Health Care 2006 Royal 23 31Documento10 páginasQual Saf Health Care 2006 Royal 23 31Gustan AriadiAinda não há avaliações
- Emergency Training, Education and Perceived Clinical Skills For Tsunami Care Among Nurses in Banda Aceh, IndonesiaDocumento12 páginasEmergency Training, Education and Perceived Clinical Skills For Tsunami Care Among Nurses in Banda Aceh, IndonesiaGustan AriadiAinda não há avaliações
- Effect of Educational Outreach To Nurses On Tuberculosis Case Detection and Primary Care of Respiratory Illness Pragmatic ClustDocumento5 páginasEffect of Educational Outreach To Nurses On Tuberculosis Case Detection and Primary Care of Respiratory Illness Pragmatic ClustGustan AriadiAinda não há avaliações
- Clinical Outcomes of Patients Requiring Ventilatory Support in Brazilian Intensive Care Units - A Multicenter, Prospective, Cohor-2Documento39 páginasClinical Outcomes of Patients Requiring Ventilatory Support in Brazilian Intensive Care Units - A Multicenter, Prospective, Cohor-2Gustan AriadiAinda não há avaliações
- WJG 19 7129Documento10 páginasWJG 19 7129Gustan AriadiAinda não há avaliações
- Midmap DermatitisDocumento1 páginaMidmap DermatitisGustan AriadiAinda não há avaliações
- WJG 19 7129Documento10 páginasWJG 19 7129Gustan AriadiAinda não há avaliações
- Clinical Outcomes of Patients Requiring Ventilatory Support in Brazilian Intensive Care Units - A Multicenter, Prospective, Cohor-2Documento39 páginasClinical Outcomes of Patients Requiring Ventilatory Support in Brazilian Intensive Care Units - A Multicenter, Prospective, Cohor-2Gustan AriadiAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Referência Bibliográfica Trauma CraniofacialDocumento2 páginasReferência Bibliográfica Trauma CraniofacialSamira FreitasAinda não há avaliações
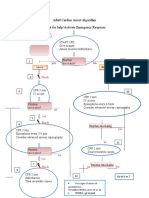
- Adult Cardiac Arrest Algorithm Shout For Help/activate Emergency ResponseDocumento1 páginaAdult Cardiac Arrest Algorithm Shout For Help/activate Emergency ResponseICU RSBMAinda não há avaliações
- Drug StudyDocumento6 páginasDrug StudyMargaret ArellanoAinda não há avaliações
- TRIAGE and MCI 083104Documento66 páginasTRIAGE and MCI 083104Nom Nom100% (1)
- DefibrilatorDocumento24 páginasDefibrilatorMoonGalaxyAinda não há avaliações
- Code Blue Running SheetDocumento2 páginasCode Blue Running Sheetenumula kumar100% (12)
- Sepsis and SirsDocumento14 páginasSepsis and SirsRuki HartawanAinda não há avaliações
- Open FractureDocumento9 páginasOpen FractureAnnyl LaurelAinda não há avaliações
- CPR ChecklistDocumento2 páginasCPR ChecklistJenny Agustin Fabros100% (2)
- BLS ChokingDocumento19 páginasBLS ChokingBernadette ArrojoAinda não há avaliações
- NABH IntroductionDocumento12 páginasNABH IntroductionKrishna100% (1)
- CPRDocumento27 páginasCPRfaizuraAinda não há avaliações
- Set Rec Pic 829Documento2 páginasSet Rec Pic 829Peter SalimAinda não há avaliações
- County Employees Salary 6-11-19Documento9 páginasCounty Employees Salary 6-11-19EffNowAinda não há avaliações
- Policy For Resuscitation TrainingDocumento54 páginasPolicy For Resuscitation TrainingSyed Mohamad Amirul SyafiqAinda não há avaliações
- Allianz - Employee Benefit GuideDocumento70 páginasAllianz - Employee Benefit GuidesanjeevnnAinda não há avaliações
- Beginner's Guide To Mechanical Ventilation PDFDocumento86 páginasBeginner's Guide To Mechanical Ventilation PDFAnonymous ZR1jT92Ez8Ainda não há avaliações
- North Central Texas Trauma Regional Advisory CouncilDocumento9 páginasNorth Central Texas Trauma Regional Advisory Councilashphoenix32Ainda não há avaliações
- U L S E C - Usls Bl1-P: Ltrasound IFE Upport Ntry OurseDocumento9 páginasU L S E C - Usls Bl1-P: Ltrasound IFE Upport Ntry Oursesaraswaty710Ainda não há avaliações
- Catalogo Philips HearthstartDocumento8 páginasCatalogo Philips HearthstartLicitaciones InbiosAinda não há avaliações
- Hospital Emergency Operations Plan TemplateDocumento53 páginasHospital Emergency Operations Plan TemplateNicholaiCabadduAinda não há avaliações
- Infant CPRDocumento1 páginaInfant CPRDaniica MacaranasAinda não há avaliações
- Microsoft PowerPoint - BHDDocumento35 páginasMicrosoft PowerPoint - BHDandarias kevinAinda não há avaliações
- PolytraumaDocumento19 páginasPolytraumaSri MahadhanaAinda não há avaliações
- HemorrhageDocumento15 páginasHemorrhageMariegreat Piscos BisnarAinda não há avaliações
- Impact of Language Barrier On Acutecaremedical Professionals Is Dependent Upon RoleDocumento4 páginasImpact of Language Barrier On Acutecaremedical Professionals Is Dependent Upon Roleravibunga4489Ainda não há avaliações
- Pre Test - Post Test BLSDocumento3 páginasPre Test - Post Test BLSChristopher AdhisasmitaAinda não há avaliações
- 7 Essential Steps of CPRDocumento2 páginas7 Essential Steps of CPRBea YmsnAinda não há avaliações
- Carnival Medical Positions DetailsDocumento6 páginasCarnival Medical Positions DetailsEliseo CastroAinda não há avaliações
- Renal Trauma: Dr. Mars Dwi Tjahjo, Sp.UDocumento21 páginasRenal Trauma: Dr. Mars Dwi Tjahjo, Sp.UbayuAinda não há avaliações