Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Community Aquired PneumoniaDocumento6 páginasCommunity Aquired PneumoniaChiro Rouy MalaluanAinda não há avaliações
- New Born ScreeningDocumento70 páginasNew Born ScreeningChiro Rouy Malaluan100% (2)
- NCP EmptyDocumento4 páginasNCP EmptyChiro Rouy MalaluanAinda não há avaliações
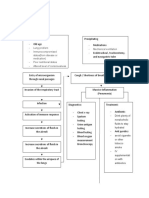
- Pathophysiology PneumoniaDocumento2 páginasPathophysiology PneumoniaChiro Rouy Malaluan100% (2)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Post Hand Spa ActivityDocumento16 páginasPost Hand Spa Activityma cleah ramos0% (1)
- ErythromycinDocumento1 páginaErythromycinKenneth Robert Abrantes0% (1)
- Tropical Splenomegaly SyndromeDocumento12 páginasTropical Splenomegaly SyndromeSaidAandySaida100% (1)
- 2017 Soal UAS - M. Operasional. - Bpk. Agustinus S PDFDocumento3 páginas2017 Soal UAS - M. Operasional. - Bpk. Agustinus S PDFraymunandarAinda não há avaliações
- Case Study On SEPSIS 2' ACP PneumoniaDocumento7 páginasCase Study On SEPSIS 2' ACP Pneumoniajcarysuitos100% (2)
- Decision Algorithm For Prescribing SGLT2 Inhibitors and GLP-1 Receptor AgonistsDocumento11 páginasDecision Algorithm For Prescribing SGLT2 Inhibitors and GLP-1 Receptor AgonistsNati BocciaAinda não há avaliações
- 2021 CPT CodesDocumento8 páginas2021 CPT CodesSundar RamanathanAinda não há avaliações
- Pressure Points - Postnatal Care Planning PDFDocumento15 páginasPressure Points - Postnatal Care Planning PDFNoraAinda não há avaliações
- Essay 3 Final DraftDocumento6 páginasEssay 3 Final Draftapi-360460383Ainda não há avaliações
- MalariaDocumento22 páginasMalariaAbdirahmanAinda não há avaliações
- Caronan NDP POLO HKGDocumento23 páginasCaronan NDP POLO HKGKatrine Danielle GuardiansAinda não há avaliações
- Social Service Providers' PerspectivesDocumento14 páginasSocial Service Providers' PerspectivesAlexander BurgaAinda não há avaliações
- Edema Por Destete Teboul - MonnetDocumento8 páginasEdema Por Destete Teboul - MonnetLuis Felipe Villamarín GranjaAinda não há avaliações
- Aging: 1) IntroductionDocumento14 páginasAging: 1) IntroductionÕbsëqúiœus Menam MikreAinda não há avaliações
- Fast Track Diagnostics Assays Brochure 0917 FINAL 1800000004342593Documento6 páginasFast Track Diagnostics Assays Brochure 0917 FINAL 1800000004342593Svasthya ManagerAinda não há avaliações
- PMID 1393911 Niacin Vs NiacinamideDocumento1 páginaPMID 1393911 Niacin Vs NiacinamideInbal LandsbergAinda não há avaliações
- Allergologists in QCDocumento4 páginasAllergologists in QCNickAinda não há avaliações
- Fundamentals of Nursing Part 5Documento36 páginasFundamentals of Nursing Part 5Honeylie Patricio100% (1)
- Medical Imaging WebquestDocumento8 páginasMedical Imaging Webquestapi-262193618Ainda não há avaliações
- President Ramon Magsaysay State University: Sagutin Mo Ko! PANUTO: Sagutin Ang Mga Sumusunod Na KatanunganDocumento4 páginasPresident Ramon Magsaysay State University: Sagutin Mo Ko! PANUTO: Sagutin Ang Mga Sumusunod Na KatanunganAndrea AngelicaAinda não há avaliações
- Intrauterine Growth Restriction IUGR Etiology andDocumento11 páginasIntrauterine Growth Restriction IUGR Etiology andFlavia Angelina SatopohAinda não há avaliações
- Triple Antibiotic PasteDocumento5 páginasTriple Antibiotic PasteVinisha Vipin SharmaAinda não há avaliações
- Quarantine and Isolation Guidance - 1.14.22Documento6 páginasQuarantine and Isolation Guidance - 1.14.22Umair Ahmed AbbasiAinda não há avaliações
- Rating Criteria: Prior To Woman'S Transfer To The DRDocumento3 páginasRating Criteria: Prior To Woman'S Transfer To The DRPatricia Ann JaringAinda não há avaliações
- Asbestos Awareness Quiz #1: AnswersDocumento2 páginasAsbestos Awareness Quiz #1: AnswersMichael NcubeAinda não há avaliações
- How To Kill Ticks On DogsDocumento3 páginasHow To Kill Ticks On DogsPhelan LoweAinda não há avaliações
- IEJ - Revitalization in EndodonticsDocumento7 páginasIEJ - Revitalization in Endodonticssoho1303Ainda não há avaliações
- Neonatal Ventilation - Neocon 2017-2Documento156 páginasNeonatal Ventilation - Neocon 2017-2RAM SOFTWARE100% (2)
- Estudo Prospectivo de Traumatismo CranioencefálicoDocumento7 páginasEstudo Prospectivo de Traumatismo CranioencefálicoCamilaAinda não há avaliações
- Urinary Tract I-WPS OfficeDocumento21 páginasUrinary Tract I-WPS Officekersameeksha borkerAinda não há avaliações