Você também pode gostar
- Muscle Injury in Repetitive Motion DisordersDocumento11 páginasMuscle Injury in Repetitive Motion DisordersAni Fran SolarAinda não há avaliações
- PAV Interacción Paciente Ventilador PDFDocumento11 páginasPAV Interacción Paciente Ventilador PDFAni Fran SolarAinda não há avaliações
- PAV y PSV PDFDocumento8 páginasPAV y PSV PDFAni Fran SolarAinda não há avaliações
- Enlightened Keyboard Technique A Definitive Model For The 21st CenturyDocumento4 páginasEnlightened Keyboard Technique A Definitive Model For The 21st CenturyAni Fran SolarAinda não há avaliações
- Traqueostomia Paciente CriticoDocumento12 páginasTraqueostomia Paciente CriticoOsman Arteaga IriarteAinda não há avaliações
- 2014 Does Immobilization After Arthroscopic Rotator Cuff Repair Increase Tendon Healing, A Systematic Review and Meta-AnalysisDocumento7 páginas2014 Does Immobilization After Arthroscopic Rotator Cuff Repair Increase Tendon Healing, A Systematic Review and Meta-AnalysisAni Fran SolarAinda não há avaliações
- 2014 The Size and Structure of Arm Movement Variability Decreased With Work Pace in A Standardised Repetitive Precision TaskDocumento13 páginas2014 The Size and Structure of Arm Movement Variability Decreased With Work Pace in A Standardised Repetitive Precision TaskAni Fran SolarAinda não há avaliações
- Paper 2Documento10 páginasPaper 2KaryTapiaLizamaAinda não há avaliações
- 2011 A Review of The Relation of Aerobic Fitness and Physical Activity To Brain Structure and Function in ChildrenDocumento11 páginas2011 A Review of The Relation of Aerobic Fitness and Physical Activity To Brain Structure and Function in ChildrenAni Fran SolarAinda não há avaliações
- 2014 Effectiveness of Continuous Vertebral Resonant Oscillation Using The POLD Method in The Treatment of Lumbar Disc Hernia. A Randomized Controlled Pilot StudyDocumento25 páginas2014 Effectiveness of Continuous Vertebral Resonant Oscillation Using The POLD Method in The Treatment of Lumbar Disc Hernia. A Randomized Controlled Pilot StudyAni Fran SolarAinda não há avaliações
- 1997 Economic Analysis of Respiratory RehabilitationDocumento10 páginas1997 Economic Analysis of Respiratory RehabilitationAni Fran SolarAinda não há avaliações
- 2001 A Focused Exercise Regimen Improves Clinical Measures of Balance in Patients With Peripheral NeuropathyDocumento5 páginas2001 A Focused Exercise Regimen Improves Clinical Measures of Balance in Patients With Peripheral NeuropathyAni Fran SolarAinda não há avaliações
- Psychobiological Model of Temperament and CharacterDocumento16 páginasPsychobiological Model of Temperament and CharacterStojan Bajraktarov100% (1)
- 2014 Rehabilitation of Meniscal Injury and SurgeryDocumento20 páginas2014 Rehabilitation of Meniscal Injury and SurgeryAni Fran SolarAinda não há avaliações
- 2013 A Systematic Review and Meta-Analysis of Tai Chi For Osteoarthritis of The KneeDocumento11 páginas2013 A Systematic Review and Meta-Analysis of Tai Chi For Osteoarthritis of The KneeAni Fran SolarAinda não há avaliações
- 2014 Electromyographic Analysis of Shoulder Muscles During Press-Up Variations and ProgressionsDocumento7 páginas2014 Electromyographic Analysis of Shoulder Muscles During Press-Up Variations and ProgressionsAni Fran SolarAinda não há avaliações
- 2001 Proprioceptive Training and Prevention of Anterior Cruciate Ligament Injuries in SoccerDocumento6 páginas2001 Proprioceptive Training and Prevention of Anterior Cruciate Ligament Injuries in SoccerAni Fran SolarAinda não há avaliações
- 2014 No. 5 Effects of Exercise Interventions On Pro-Inflammatory Biomarkers in Breast Cancer SurvivorsDocumento1 página2014 No. 5 Effects of Exercise Interventions On Pro-Inflammatory Biomarkers in Breast Cancer SurvivorsAni Fran SolarAinda não há avaliações
- 2014 Walking Energetics, Fatigability, and Fatigue in Older Adults The Study of Energy and Aging PilotDocumento8 páginas2014 Walking Energetics, Fatigability, and Fatigue in Older Adults The Study of Energy and Aging PilotAni Fran SolarAinda não há avaliações
- 2001 An Economic Overview of Chronic Obstructive Pulmonary DiseaseDocumento20 páginas2001 An Economic Overview of Chronic Obstructive Pulmonary DiseaseAni Fran SolarAinda não há avaliações
- Variability in Action, Contributions of A Songbird Cortical-Basal Ganglia Circuit To Vocal Motor Learning and ControlDocumento9 páginasVariability in Action, Contributions of A Songbird Cortical-Basal Ganglia Circuit To Vocal Motor Learning and ControlAni Fran SolarAinda não há avaliações
- 2011 A Review of The Relation of Aerobic Fitness and Physical Activity To Brain Structure and Function in ChildrenDocumento11 páginas2011 A Review of The Relation of Aerobic Fitness and Physical Activity To Brain Structure and Function in ChildrenAni Fran SolarAinda não há avaliações
- 2003 How We Walk, Central Control of Muscle Activity During Human WalkingDocumento11 páginas2003 How We Walk, Central Control of Muscle Activity During Human WalkingAni Fran SolarAinda não há avaliações
- 2014 Effectiveness of Continuous Vertebral Resonant Oscillation Using The POLD Method in The Treatment of Lumbar Disc Hernia. A Randomized Controlled Pilot StudyDocumento25 páginas2014 Effectiveness of Continuous Vertebral Resonant Oscillation Using The POLD Method in The Treatment of Lumbar Disc Hernia. A Randomized Controlled Pilot StudyAni Fran SolarAinda não há avaliações
- Differential Activation of Parts of The Serratus Anterior Muscle During Push-UpDocumento7 páginasDifferential Activation of Parts of The Serratus Anterior Muscle During Push-UpRudolfGerAinda não há avaliações
- 2014 Factors Affecting Rotator Cuff HealingDocumento11 páginas2014 Factors Affecting Rotator Cuff HealingAni Fran SolarAinda não há avaliações
- 2014 Evaluating Anterior Knee PainDocumento21 páginas2014 Evaluating Anterior Knee PainAni Fran SolarAinda não há avaliações
- 2014 O1-16-6 Center-Based Exercise On Cancer-Related Fatigue in Breast Cancer Survivors During Active Treatment A Meta-AnalysisDocumento1 página2014 O1-16-6 Center-Based Exercise On Cancer-Related Fatigue in Breast Cancer Survivors During Active Treatment A Meta-AnalysisAni Fran SolarAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- WorkoutDocumento6 páginasWorkoutapi-389190950Ainda não há avaliações
- The Innervation of The Soft Palate MusclesDocumento7 páginasThe Innervation of The Soft Palate MusclesjmccoyAinda não há avaliações
- Spinal TraumaDocumento81 páginasSpinal TraumaharilAinda não há avaliações
- Back RubDocumento18 páginasBack RubJehan EnokAinda não há avaliações
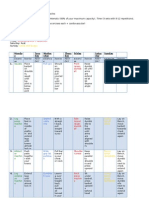
- Fitt PlanDocumento5 páginasFitt Planapi-301804120Ainda não há avaliações
- 7D Hifu HF700Documento49 páginas7D Hifu HF700Jonathan AvilesAinda não há avaliações
- Ankle Rehab Exercises GuideDocumento4 páginasAnkle Rehab Exercises GuideHazel Grace LancasterAinda não há avaliações
- Anatomy 090819Documento30 páginasAnatomy 090819Vaishnavi GourabathiniAinda não há avaliações
- Gorilla WorkoutDocumento4 páginasGorilla WorkoutKishoreVancheeshwaranAinda não há avaliações
- OSCE Checklist GALS ExaminationDocumento2 páginasOSCE Checklist GALS ExaminationMohammed Mostafa KhalifaAinda não há avaliações
- Lab Exercise No. 5: X-Ray Identification Activity: Name: Rocel Marie D. Lopez Section: BSN 1105Documento11 páginasLab Exercise No. 5: X-Ray Identification Activity: Name: Rocel Marie D. Lopez Section: BSN 1105Rocel Marie Lopez100% (1)
- People Ke. Africa and The Western Pacifi People (WHODocumento74 páginasPeople Ke. Africa and The Western Pacifi People (WHOMoemoe NyanAinda não há avaliações
- Groin Strain Rehabilitation PDFDocumento3 páginasGroin Strain Rehabilitation PDFOscar NgAinda não há avaliações
- Muscle Tone PhysiologyDocumento5 páginasMuscle Tone PhysiologyfatimaAinda não há avaliações
- ALVINA Research-1Documento3 páginasALVINA Research-1Alvina MudyandariAinda não há avaliações
- Neurological ExamDocumento6 páginasNeurological ExamTiti Daraban100% (2)
- New Neet 2020 - Watermarked PDFDocumento11 páginasNew Neet 2020 - Watermarked PDFAnangsha DattaAinda não há avaliações
- Somatom Emotion 6 SpecialDocumento98 páginasSomatom Emotion 6 SpecialGabriel PaucarAinda não há avaliações
- Body PartsDocumento2 páginasBody PartsVictor BarbosaAinda não há avaliações
- STOMACHDocumento20 páginasSTOMACHChoudhary FahadAinda não há avaliações
- 22 Respiratory SystemDocumento99 páginas22 Respiratory SystemvanderphysAinda não há avaliações
- Male puberty body mapDocumento2 páginasMale puberty body mapDOMINGO HENG-GE CHUAAinda não há avaliações
- 5x5 Jump Program by Bill StarrDocumento8 páginas5x5 Jump Program by Bill StarrColin ChungAinda não há avaliações
- New Microsoft Word DocumentDocumento13 páginasNew Microsoft Word DocumentdinaAinda não há avaliações
- ASSESSING THE NEUROLOGICAL SYSTEM ChecklistDocumento4 páginasASSESSING THE NEUROLOGICAL SYSTEM ChecklistCyril Dayne Marie BaldeAinda não há avaliações
- The Respiratory System (Handouts)Documento6 páginasThe Respiratory System (Handouts)EdAinda não há avaliações
- Metabolism of Human DiseasesDocumento382 páginasMetabolism of Human DiseasesLari H.Ainda não há avaliações
- PEX-09-01 GGGDocumento4 páginasPEX-09-01 GGGDjalika.zAinda não há avaliações
- Scapula Fracture: DR Jaseem ShamsudeenDocumento32 páginasScapula Fracture: DR Jaseem ShamsudeenJaseemshams ThottiyilAinda não há avaliações
- Anatomy Physio ExamDocumento2 páginasAnatomy Physio ExamJecxter BedañaAinda não há avaliações