Você também pode gostar
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- A Critical Appreciation of Ode To NightingaleDocumento3 páginasA Critical Appreciation of Ode To NightingaleBaloch Karawan100% (2)
- Maxillofacial Notes DR - Mahmoud RamadanDocumento83 páginasMaxillofacial Notes DR - Mahmoud Ramadanaziz200775% (4)
- Alugbati Plant Pigment Extraction As Natural Watercolor SourceDocumento6 páginasAlugbati Plant Pigment Extraction As Natural Watercolor SourceMike Arvin Serrano100% (1)
- Business Plan Example - Little LearnerDocumento26 páginasBusiness Plan Example - Little LearnerCourtney mcintosh100% (1)
- Refinería Kirkuk PDFDocumento11 páginasRefinería Kirkuk PDFcesarinarragaAinda não há avaliações
- Itc LimitedDocumento64 páginasItc Limitedjulee G0% (1)
- Latest Low NOx Combustion TechnologyDocumento7 páginasLatest Low NOx Combustion Technology95113309Ainda não há avaliações
- LifesaverDocumento14 páginasLifesaverAnang FajarAinda não há avaliações
- Phys Ther 2012 Macedo 363 77Documento18 páginasPhys Ther 2012 Macedo 363 77Anang FajarAinda não há avaliações
- Af Af: Aka Aka Aka Aka Aka AkaDocumento3 páginasAf Af: Aka Aka Aka Aka Aka AkaAnang FajarAinda não há avaliações
- Minggu Ke-5 Bulan Maret 2018Documento3 páginasMinggu Ke-5 Bulan Maret 2018Anang FajarAinda não há avaliações
- Phys Ther 2012 Opheim 279 88Documento12 páginasPhys Ther 2012 Opheim 279 88Anang FajarAinda não há avaliações
- Reproduction of Overall Spontaneous Pain Pattern by Manual Stimulation of Active Myofascial Trigger Points in Fibromyalgia PatientsDocumento7 páginasReproduction of Overall Spontaneous Pain Pattern by Manual Stimulation of Active Myofascial Trigger Points in Fibromyalgia PatientsAnang FajarAinda não há avaliações
- Fibro 4Documento3 páginasFibro 4Anang FajarAinda não há avaliações
- Phys Ther 2012 Ioppolo 1376 85Documento12 páginasPhys Ther 2012 Ioppolo 1376 85Anang FajarAinda não há avaliações
- 13 585aDocumento2 páginas13 585aAnang FajarAinda não há avaliações
- Rhs 15Documento8 páginasRhs 15Anang FajarAinda não há avaliações
- Rhs 15Documento8 páginasRhs 15Anang FajarAinda não há avaliações
- CH02 SampleDocumento26 páginasCH02 SampleAnang FajarAinda não há avaliações
- Referred From Orthopaedic Outpatient Clinic With Neglected Dislocation Elbow S Post Open ReductionDocumento1 páginaReferred From Orthopaedic Outpatient Clinic With Neglected Dislocation Elbow S Post Open ReductionAnang FajarAinda não há avaliações
- Referred From Orthopaedic Outpatient Clinic With Neglected Dislocation Elbow S Post Open ReductionDocumento1 páginaReferred From Orthopaedic Outpatient Clinic With Neglected Dislocation Elbow S Post Open ReductionAnang FajarAinda não há avaliações
- Cervical Root Syndrome Sc4Documento50 páginasCervical Root Syndrome Sc4Anang FajarAinda não há avaliações
- Rehabilitation of Overhead Shoulder InjuriesDocumento3 páginasRehabilitation of Overhead Shoulder InjuriesAnang FajarAinda não há avaliações
- Referral of Medical Rehabilitation Hospital Poly Pamekasan With BellDocumento1 páginaReferral of Medical Rehabilitation Hospital Poly Pamekasan With BellAnang FajarAinda não há avaliações
- Referred From Orthopaedic Outpatient Clinic With Neglected Dislocation Elbow S Post Open ReductionDocumento1 páginaReferred From Orthopaedic Outpatient Clinic With Neglected Dislocation Elbow S Post Open ReductionAnang FajarAinda não há avaliações
- Referral of Medical Rehabilitation Hospital Poly Pamekasan With BellDocumento1 páginaReferral of Medical Rehabilitation Hospital Poly Pamekasan With BellAnang FajarAinda não há avaliações
- Cervical Root SyndromeDocumento48 páginasCervical Root SyndromeAnang FajarAinda não há avaliações
- Ankle Tendon InjuryDocumento7 páginasAnkle Tendon InjuryAnang FajarAinda não há avaliações
- Pre Conditioning ExerciseDocumento24 páginasPre Conditioning ExerciseAnang FajarAinda não há avaliações
- Imaging Anterior Cruciate Ligament Tear - Helpful Tips Imaging Anterior Cruciate Ligament Tear - Helpful TipsDocumento5 páginasImaging Anterior Cruciate Ligament Tear - Helpful Tips Imaging Anterior Cruciate Ligament Tear - Helpful TipsAnang FajarAinda não há avaliações
- De Quervain's Tenosynovitis: By: Dr. HermilawatyDocumento35 páginasDe Quervain's Tenosynovitis: By: Dr. HermilawatyAnang FajarAinda não há avaliações
- Trigger Finger: By:Ida Yuanita, MDDocumento33 páginasTrigger Finger: By:Ida Yuanita, MDAnang FajarAinda não há avaliações
- Rehabilitation After ACL ReconstructionDocumento4 páginasRehabilitation After ACL ReconstructionAnang FajarAinda não há avaliações
- Lateral Epicondylitis (Tennis Elbow) : By:Ida Yuanita, MDDocumento37 páginasLateral Epicondylitis (Tennis Elbow) : By:Ida Yuanita, MDAnang FajarAinda não há avaliações
- Carpal Tunnel Syndrome: by A. A. Sagung Mas CahyandariDocumento37 páginasCarpal Tunnel Syndrome: by A. A. Sagung Mas CahyandariAnang FajarAinda não há avaliações
- Biomechanics and MOI of The AnkleDocumento37 páginasBiomechanics and MOI of The AnkleAnang FajarAinda não há avaliações
- NG Teng Fong Discharge DocumentsDocumento14 páginasNG Teng Fong Discharge DocumentsAnonymous yGwMIPJRawAinda não há avaliações
- Enviroline 2405: Hybrid EpoxyDocumento4 páginasEnviroline 2405: Hybrid EpoxyMuthuKumarAinda não há avaliações
- G1 Series User Manual Ver. 1.2Documento101 páginasG1 Series User Manual Ver. 1.2unedo parhusip100% (1)
- Organogram - Qa / QC: Srinivasan SrinivasanDocumento4 páginasOrganogram - Qa / QC: Srinivasan SrinivasanGowtham VenkatAinda não há avaliações
- AFMAN91-201 NewDocumento458 páginasAFMAN91-201 NewbombtechAinda não há avaliações
- Science and TechnologyDocumento21 páginasScience and TechnologyPat MillerAinda não há avaliações
- Offender TypologiesDocumento8 páginasOffender TypologiesSahil AnsariAinda não há avaliações
- Topic of Assignment: Health Wellness and Yoga AssignmentDocumento12 páginasTopic of Assignment: Health Wellness and Yoga AssignmentHarsh XAinda não há avaliações
- 'Bubble Kid' Success Puts Gene Therapy Back On TrackDocumento5 páginas'Bubble Kid' Success Puts Gene Therapy Back On TrackAbby Grey Lopez100% (1)
- Scope: Procter and GambleDocumento30 páginasScope: Procter and GambleIrshad AhamedAinda não há avaliações
- READING 4 UNIT 8 Crime-Nurse Jorge MonarDocumento3 páginasREADING 4 UNIT 8 Crime-Nurse Jorge MonarJORGE ALEXANDER MONAR BARRAGANAinda não há avaliações
- Ras Shastra PPT 6Documento10 páginasRas Shastra PPT 6Soham BhureAinda não há avaliações
- Characteristics of Testable HypothesesDocumento30 páginasCharacteristics of Testable HypothesesMarivic Diano67% (3)
- Dr. Sajjad Hussain Sumrra Isomerism (CHEM-305) Inorganic Chemistry-IIDocumento48 páginasDr. Sajjad Hussain Sumrra Isomerism (CHEM-305) Inorganic Chemistry-IITanya DilshadAinda não há avaliações
- Lab Manual PDFDocumento68 páginasLab Manual PDFSantino AwetAinda não há avaliações
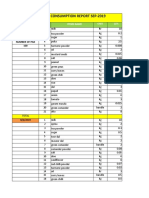
- Daily Staff Food Consumption Reports Sep-2019Documento4 páginasDaily Staff Food Consumption Reports Sep-2019Manjit RawatAinda não há avaliações
- Maintenance Instructions, Parts Identification & Seal Kits For Series 2H / 2HD / 2HB & 3H / 3HD / 3HBDocumento10 páginasMaintenance Instructions, Parts Identification & Seal Kits For Series 2H / 2HD / 2HB & 3H / 3HD / 3HBAtaa AssaadAinda não há avaliações
- Inverter 1 KW ManualDocumento44 páginasInverter 1 KW ManualLeonardoAinda não há avaliações
- Sanctuary Policy PomonaDocumento3 páginasSanctuary Policy PomonaGabriel EliasAinda não há avaliações
- IPG Or-01 - PTC Train Infrastructure Electrical Safety RulesDocumento50 páginasIPG Or-01 - PTC Train Infrastructure Electrical Safety Rules4493464Ainda não há avaliações
- High Speed DoorsDocumento64 páginasHigh Speed DoorsVadimMedooffAinda não há avaliações
- Demages Goods RecordDocumento22 páginasDemages Goods Recordtariq malikAinda não há avaliações
- Women EmpowermentDocumento7 páginasWomen EmpowermentJessica Glenn100% (1)