Você também pode gostar
- Pros Exam 1 2002Documento8 páginasPros Exam 1 2002mirfanulhaqAinda não há avaliações
- 2 Saliva PhysiologyDocumento20 páginas2 Saliva PhysiologyvelangniAinda não há avaliações
- Alveolar bone formation and structureDocumento16 páginasAlveolar bone formation and structuremirfanulhaqAinda não há avaliações
- Pros QuestionsDocumento7 páginasPros QuestionsmirfanulhaqAinda não há avaliações
- Fundamentals of SalivaDocumento15 páginasFundamentals of SalivasreedamAinda não há avaliações
- Oral InfectionsDocumento14 páginasOral InfectionsmirfanulhaqAinda não há avaliações
- Pros Exam 1 2003Documento8 páginasPros Exam 1 2003mirfanulhaqAinda não há avaliações
- Gingival InflammationDocumento19 páginasGingival InflammationmirfanulhaqAinda não há avaliações
- Comprehensive Periodontal Exam GuideDocumento40 páginasComprehensive Periodontal Exam GuideKavin SandhuAinda não há avaliações
- Management of Cracked TeethDocumento6 páginasManagement of Cracked Teethsaifuddin suhri100% (2)
- Peds Restorative PDFDocumento4 páginasPeds Restorative PDFmirfanulhaqAinda não há avaliações
- Adhesion SystemsDocumento13 páginasAdhesion SystemsTolean AndreeviciAinda não há avaliações
- Pros Exam 1 2002Documento8 páginasPros Exam 1 2002mirfanulhaqAinda não há avaliações
- Anticoagulation GuidelinesDocumento2 páginasAnticoagulation GuidelinesmirfanulhaqAinda não há avaliações
- Pulp Protection Methods and MaterialsDocumento13 páginasPulp Protection Methods and MaterialsmirfanulhaqAinda não há avaliações
- Wound Healing PDFDocumento7 páginasWound Healing PDFmirfanulhaqAinda não há avaliações
- Oral Healthcare Considerations For The Pregnant WomanDocumento4 páginasOral Healthcare Considerations For The Pregnant WomanmirfanulhaqAinda não há avaliações
- Complications in Dentoalveolar Surgery PDFDocumento37 páginasComplications in Dentoalveolar Surgery PDFmirfanulhaqAinda não há avaliações
- Making Sense of Mouth Ulceration 6Documento3 páginasMaking Sense of Mouth Ulceration 6mirfanulhaqAinda não há avaliações
- Making Sense of Mouth Ulceration 6Documento3 páginasMaking Sense of Mouth Ulceration 6mirfanulhaqAinda não há avaliações
- Guide to Fluoride TherapyDocumento4 páginasGuide to Fluoride TherapymirfanulhaqAinda não há avaliações
- Pulp 2008 HandoutDocumento7 páginasPulp 2008 HandoutNemanja MiticAinda não há avaliações
- Pulp Protection Methods and MaterialsDocumento13 páginasPulp Protection Methods and MaterialsmirfanulhaqAinda não há avaliações
- Making Sense of Mouth Ulceration 5Documento3 páginasMaking Sense of Mouth Ulceration 5mirfanulhaqAinda não há avaliações
- Making Sense of Mouth Ulceration 3Documento4 páginasMaking Sense of Mouth Ulceration 3mirfanulhaqAinda não há avaliações
- Making Sense of Mouth Ulceration 4Documento4 páginasMaking Sense of Mouth Ulceration 4mirfanulhaqAinda não há avaliações
- Scully Oral UlcersDocumento3 páginasScully Oral UlcersdeenmAinda não há avaliações
- Scully Oral UlcersDocumento3 páginasScully Oral UlcersdeenmAinda não há avaliações
- Scully Oral UlcersDocumento3 páginasScully Oral UlcersdeenmAinda não há avaliações
- Opath - Most Common ListDocumento4 páginasOpath - Most Common ListmirfanulhaqAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Duaa Salih Makawi SonDocumento25 páginasDuaa Salih Makawi Sonnnawaz4Ainda não há avaliações
- Endodontic InsrumentDocumento52 páginasEndodontic InsrumentSawsan Z. JwaiedAinda não há avaliações
- Apexogenesis of An Immature Permanent Molar With The Use of Er, Cr:Ysgg Laser and Mineral Trioxide AggregateDocumento4 páginasApexogenesis of An Immature Permanent Molar With The Use of Er, Cr:Ysgg Laser and Mineral Trioxide AggregateEseman DentalAinda não há avaliações
- Removable Orthodontic Appliances - VijayalakshmiDocumento104 páginasRemovable Orthodontic Appliances - Vijayalakshmidrkamesh75% (8)
- Use of Chlorhexidine Varnishes in Preventing and Treating Periodontal DiseaseDocumento4 páginasUse of Chlorhexidine Varnishes in Preventing and Treating Periodontal Diseasetaher adelAinda não há avaliações
- Operative Dentistry: Restoring Primary TeethDocumento35 páginasOperative Dentistry: Restoring Primary TeethNoor AlsanouriAinda não há avaliações
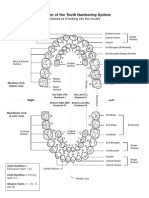
- Diagram of The Tooth Numbering SystemDocumento1 páginaDiagram of The Tooth Numbering Systemsaleh900Ainda não há avaliações
- The Daughter Test in Aesthetic or Cosmetic DentiDocumento8 páginasThe Daughter Test in Aesthetic or Cosmetic DentiRay ChaoAinda não há avaliações
- Evaluation of The Effects of The Hybrid Pendulum in Comparison With The Conventional Pendulum ApplianceDocumento8 páginasEvaluation of The Effects of The Hybrid Pendulum in Comparison With The Conventional Pendulum ApplianceARIANA AMARILES BAENAAinda não há avaliações
- Condiciones ParticularesDocumento19 páginasCondiciones ParticularesBlaise BowlyAinda não há avaliações
- Angkatan 8 Prodi PPDGS Ilmu Bedah Mulut Dan Maksilofasial Universitas Hasanuddin MakassarDocumento16 páginasAngkatan 8 Prodi PPDGS Ilmu Bedah Mulut Dan Maksilofasial Universitas Hasanuddin Makassarreyhan1Ainda não há avaliações
- Removable Prosthodontics: Louis Blatterfein S. Howard PayneDocumento6 páginasRemovable Prosthodontics: Louis Blatterfein S. Howard PayneArjun NarangAinda não há avaliações
- Cleft Lip & Palate Care GuideDocumento10 páginasCleft Lip & Palate Care GuideFarhaana ShaboodienAinda não há avaliações
- Adult Orthodontics SeminarDocumento52 páginasAdult Orthodontics Seminaravanthika krishnaraj100% (2)
- Classification of ArticulatorsDocumento4 páginasClassification of ArticulatorsRishiraj Jaiswal67% (3)
- Oral Surgery 14874Documento4 páginasOral Surgery 14874StanislavNemtanuAinda não há avaliações
- Treatment Impaksi M1 Dengan Removable Appliance PDFDocumento7 páginasTreatment Impaksi M1 Dengan Removable Appliance PDFTokubetsu VidadiAinda não há avaliações
- An Alternative Approach For The Mainframe of Flabby Ridge ©2019Documento3 páginasAn Alternative Approach For The Mainframe of Flabby Ridge ©2019DrAhmed HamzaAinda não há avaliações
- Definition: Purpose: Equipment NeededDocumento3 páginasDefinition: Purpose: Equipment NeededKim VillacorteAinda não há avaliações
- Ada & AnsiDocumento24 páginasAda & Ansikermink100% (3)
- Lec 4 Prosthodontics PDFDocumento7 páginasLec 4 Prosthodontics PDFmustafa7calligrapherAinda não há avaliações
- Ledging and Blockage of Root Canals During Canal Preparation: Causes, Recognition, Prevention, Management, and OutcomesDocumento21 páginasLedging and Blockage of Root Canals During Canal Preparation: Causes, Recognition, Prevention, Management, and Outcomesgemis96Ainda não há avaliações
- Final StomatologyDocumento49 páginasFinal StomatologyRehema MulewaAinda não há avaliações
- CROSSBITE According To GraberDocumento29 páginasCROSSBITE According To GraberAslamCv100% (1)
- New Icon 8pg BrochureDocumento8 páginasNew Icon 8pg BrochureMiruna Maria MiulescuAinda não há avaliações
- Canine Impaction Different MethodsDocumento11 páginasCanine Impaction Different MethodsMSHAinda não há avaliações
- Surgical Guides PDFDocumento8 páginasSurgical Guides PDFjagjit singhAinda não há avaliações
- Significance of Dental Anatomy, Histology, Physiology, and Occlusion (L1)Documento54 páginasSignificance of Dental Anatomy, Histology, Physiology, and Occlusion (L1)Jarrah LumpayAinda não há avaliações
- Chronic Marginal PeriodontitisDocumento21 páginasChronic Marginal PeriodontitisLaslo Mihaela Larisa100% (1)
- Parameters of Care Supplement: Parameter On "Refractory" PeriodontitisDocumento2 páginasParameters of Care Supplement: Parameter On "Refractory" PeriodontitisEllis E. RamadianAinda não há avaliações