Você também pode gostar
- A Guide to Diabetes: Symptoms; Causes; Treatment; PreventionNo EverandA Guide to Diabetes: Symptoms; Causes; Treatment; PreventionAinda não há avaliações
- 2004-Case Study Diabetes in A Patient With Cirrhosis PDFDocumento5 páginas2004-Case Study Diabetes in A Patient With Cirrhosis PDFAnugrah ElfaAinda não há avaliações
- Diabetes Mellitus IIDocumento20 páginasDiabetes Mellitus IIMa R Dy100% (1)
- Clinical Management of Diabetes in The Elderly: Practical PointersDocumento4 páginasClinical Management of Diabetes in The Elderly: Practical Pointersannaafia69969Ainda não há avaliações
- Biochemical Markers On CH and DMT2 Yenny PAGDDocumento41 páginasBiochemical Markers On CH and DMT2 Yenny PAGDdithaAinda não há avaliações
- Alternative Therapies For DM 2Documento14 páginasAlternative Therapies For DM 2Ferc27Ainda não há avaliações
- DM FinaDocumento3 páginasDM FinaChared LumbaAinda não há avaliações
- Dr. Rasha Salama: PHD Public Health, Suez Canal University, Egypt Diabetes MSC, Cardiff University, United KingdomDocumento37 páginasDr. Rasha Salama: PHD Public Health, Suez Canal University, Egypt Diabetes MSC, Cardiff University, United Kingdomdwi istutikAinda não há avaliações
- Definition of Diabetes Mellitus (DM)Documento12 páginasDefinition of Diabetes Mellitus (DM)Romarc Owen CorpuzAinda não há avaliações
- HypoglycemiaDocumento19 páginasHypoglycemiaJesus PadillaAinda não há avaliações
- Dental Management of Patients With Diabetes MellitusDocumento8 páginasDental Management of Patients With Diabetes Mellitusاحمد سلامAinda não há avaliações
- Curs Studenti StrainiDocumento71 páginasCurs Studenti StrainiAlexandru VisanAinda não há avaliações
- CKD Dan DM (Modul 4)Documento6 páginasCKD Dan DM (Modul 4)Nurul AwaliahAinda não há avaliações
- CaseDocumento7 páginasCaseDenny EmiliusAinda não há avaliações
- Diabetes and Cardiovascular Disease: Story of DiscoveryDocumento5 páginasDiabetes and Cardiovascular Disease: Story of DiscoveryMahesh DmAinda não há avaliações
- DD Metabolic SyndromeDocumento5 páginasDD Metabolic SyndromeEluAinda não há avaliações
- Katarak DM RemajaDocumento8 páginasKatarak DM RemajaHIstoryAinda não há avaliações
- Diabetes For Dentists: DR Jackie Elliott Clinical Lecturer in DiabetesDocumento37 páginasDiabetes For Dentists: DR Jackie Elliott Clinical Lecturer in DiabetesKevalChavdaAinda não há avaliações
- Diabetes in Palliative Care CompletedDocumento4 páginasDiabetes in Palliative Care Completedaya PermatasariAinda não há avaliações
- Ald & MasldDocumento19 páginasAld & MasldAli SafaaAinda não há avaliações
- Chronic Kidney Disease Case StudyDocumento52 páginasChronic Kidney Disease Case StudyGi100% (1)
- Symptoms of HypoglycemiaDocumento20 páginasSymptoms of Hypoglycemiakenny StefAinda não há avaliações
- Diabetes Mellitus: Group 3ADocumento8 páginasDiabetes Mellitus: Group 3AAradhanaRamchandaniAinda não há avaliações
- Screening: DM Tipe 1 Practice EssentialsDocumento20 páginasScreening: DM Tipe 1 Practice Essentialskuchaibaru90Ainda não há avaliações
- Diabetes Mellitus: (DM)Documento84 páginasDiabetes Mellitus: (DM)Andika HAinda não há avaliações
- Meds DiabetesDocumento5 páginasMeds DiabetesAnjangsari 'aRie' WijayantiAinda não há avaliações
- Medical Abbreviation For Diabetes Mellitus With Endocrine System Abbreviation Medical Term Meaning / DefinitionDocumento26 páginasMedical Abbreviation For Diabetes Mellitus With Endocrine System Abbreviation Medical Term Meaning / DefinitionCt AinnAinda não há avaliações
- Title: HypoglycemiaDocumento13 páginasTitle: Hypoglycemia025 MUHAMAD HAZIQ BIN AHMAD AZMANAinda não há avaliações
- Management of Blood GlucoseDocumento8 páginasManagement of Blood GlucoseerwanAinda não há avaliações
- Diabetes Mellitus-Chronic ComplicationsDocumento12 páginasDiabetes Mellitus-Chronic ComplicationsAnam MirAinda não há avaliações
- Diabetes Mellitus: Is Type Surgical Disease?Documento10 páginasDiabetes Mellitus: Is Type Surgical Disease?Mateo TamayoAinda não há avaliações
- Kimmelstiel-Wilson Syndrome BDocumento13 páginasKimmelstiel-Wilson Syndrome BRanela Kwinkee Pastor SalazarAinda não há avaliações
- دبلومةDocumento44 páginasدبلومةlight tweenAinda não há avaliações
- Diabetic Ketoacidosis in Toddler With A Diaper RashDocumento4 páginasDiabetic Ketoacidosis in Toddler With A Diaper RashKarl Angelo MontanoAinda não há avaliações
- Diagnosis and Management of Type 2 Diabetes Mellitus ©stephen D. Sisson MD/Ambulatory Curriculum 2021Documento48 páginasDiagnosis and Management of Type 2 Diabetes Mellitus ©stephen D. Sisson MD/Ambulatory Curriculum 2021Carolina González RiveraAinda não há avaliações
- Case Study: Screening and Treatment of Pre-Diabetes in Primary CareDocumento7 páginasCase Study: Screening and Treatment of Pre-Diabetes in Primary CareEnzo EnzowzowAinda não há avaliações
- Diabetes Tipe 2Documento6 páginasDiabetes Tipe 2Cornelia MonicaAinda não há avaliações
- Diabetes Mellitus - 2022-2023 - First Semester - DownloadDocumento97 páginasDiabetes Mellitus - 2022-2023 - First Semester - DownloadLeoAinda não há avaliações
- Chir 1Documento9 páginasChir 1George MogaAinda não há avaliações
- British Journal of Diabetes & Vascular Disease-2006-Pratley-150-6Documento8 páginasBritish Journal of Diabetes & Vascular Disease-2006-Pratley-150-6Nurul FajrinaAinda não há avaliações
- Diabetes PPT FianlDocumento31 páginasDiabetes PPT FianlUqba MishalAinda não há avaliações
- Pathology of Type 2 DiabetesDocumento4 páginasPathology of Type 2 DiabetesJenny SembranoAinda não há avaliações
- DM Type 2 Practice EssentialsDocumento31 páginasDM Type 2 Practice Essentialskuchaibaru90Ainda não há avaliações
- Type 2 Diabetes MellitusDocumento24 páginasType 2 Diabetes Mellitusdr. M.F. Romdhoni100% (1)
- Insulin Secretion and FunctionDocumento8 páginasInsulin Secretion and FunctionWendy EscalanteAinda não há avaliações
- Mellitus/ Section 1: Epidemiology and AetiologyDocumento52 páginasMellitus/ Section 1: Epidemiology and AetiologybimackpbgtAinda não há avaliações
- Hipertensi: Am Fam Physician. 2014 Oct 1 90 (7) :503-504Documento5 páginasHipertensi: Am Fam Physician. 2014 Oct 1 90 (7) :503-504Alexander TegarAinda não há avaliações
- Diabetes in PregnancyDocumento14 páginasDiabetes in Pregnancywalaaahmed213Ainda não há avaliações
- Diabetes Mellitus: Zenebe N. (B Pharm, M Pharm) May, 2022Documento93 páginasDiabetes Mellitus: Zenebe N. (B Pharm, M Pharm) May, 2022The AbyssinicansAinda não há avaliações
- Lecture 1 Carbohydrate 1Documento39 páginasLecture 1 Carbohydrate 1mer12sswAinda não há avaliações
- Glucosa 2012Documento6 páginasGlucosa 2012martynbbAinda não há avaliações
- Diabetes: Introduction and History of The Diabetes MellitusDocumento6 páginasDiabetes: Introduction and History of The Diabetes Mellitusثہيہودور'ۦ شہوأنہﮩٰۧٛۗ ﮩٰۧٛAinda não há avaliações
- Type 2 Diabetes MellitusDocumento19 páginasType 2 Diabetes MellitusFelipe Senn Guerrero100% (2)
- Diabetes: in All Asymptomatic People Whose Initial Result Suggests A Diagnosis of Diabetes, A ConfirmatoryDocumento3 páginasDiabetes: in All Asymptomatic People Whose Initial Result Suggests A Diagnosis of Diabetes, A ConfirmatorytothomileAinda não há avaliações
- Jurnal:: Fulminant Type 1 Diabetes Mellitus (A Case Report)Documento10 páginasJurnal:: Fulminant Type 1 Diabetes Mellitus (A Case Report)Forensik UMIAinda não há avaliações
- Pancreatic Diabetes Mellitus: Frequency and DiagnosisDocumento10 páginasPancreatic Diabetes Mellitus: Frequency and Diagnosisbalthier37Ainda não há avaliações
- Relapsing and Remitting Insulin Requiring Diabetes: Type 1 or Type 2?Documento2 páginasRelapsing and Remitting Insulin Requiring Diabetes: Type 1 or Type 2?Linda NoveraAinda não há avaliações
- Cleveland Clinic Journal of Medicine 2009 SHRISHRIMAL 649 55Documento7 páginasCleveland Clinic Journal of Medicine 2009 SHRISHRIMAL 649 55คุณนาย เหม่เกว่Ainda não há avaliações
- Diabetes Mellitus HospitalDocumento29 páginasDiabetes Mellitus HospitalgegeAinda não há avaliações
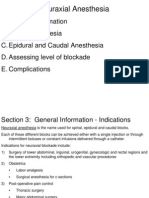
- Sab - Caudal EpiduralDocumento23 páginasSab - Caudal EpiduralAlfita InnayatiAinda não há avaliações
- Case Study: Diabetes in A Patient With Cirrhosis: PresentationDocumento5 páginasCase Study: Diabetes in A Patient With Cirrhosis: PresentationJohanLazuardiAinda não há avaliações
- Difficult AirwayDocumento9 páginasDifficult AirwaySteve JohnstoneAinda não há avaliações
- Central Venous Pressure and Pulmonary Capillary Wedge Pressure MonitoringDocumento6 páginasCentral Venous Pressure and Pulmonary Capillary Wedge Pressure MonitoringSuresh KumarAinda não há avaliações
- Retinal DetachmentDocumento8 páginasRetinal DetachmentJohanLazuardiAinda não há avaliações
- Chapter 09: Photo Atlas of Drug Administration Test Bank: Multiple ChoiceDocumento8 páginasChapter 09: Photo Atlas of Drug Administration Test Bank: Multiple ChoicePrettygirl716Ainda não há avaliações
- MEDINA PoliciesDocumento51 páginasMEDINA PoliciesJessica DensingAinda não há avaliações
- OSCE Checklist VenepunctureDocumento2 páginasOSCE Checklist Venepunctureanju rachel joseAinda não há avaliações
- Hepatic EncephalopatyDocumento15 páginasHepatic EncephalopatyJariza Daryl Tamang MejiaAinda não há avaliações
- Trasturel 440mg Anti CancerDocumento3 páginasTrasturel 440mg Anti CancerRadhika ChandranAinda não há avaliações
- Peads Teacher MannualDocumento108 páginasPeads Teacher MannualMobin Ur Rehman KhanAinda não há avaliações
- 7 Medicine RheumatologyDocumento28 páginas7 Medicine RheumatologyAmitAinda não há avaliações
- Inflammatory Lesions of The JawsDocumento54 páginasInflammatory Lesions of The JawsAi Rafikah Nurpratiwi100% (1)
- Basic Life Support & Medical EmergencyDocumento39 páginasBasic Life Support & Medical EmergencyRoyle LolingAinda não há avaliações
- Nursing Care Plan Cerebrovascular Accident (CVA)Documento1 páginaNursing Care Plan Cerebrovascular Accident (CVA)deric97% (32)
- Antop Manual Workshop HandoutDocumento24 páginasAntop Manual Workshop HandoutMaBinAinda não há avaliações
- Community Patient Education Preparation ProjectDocumento2 páginasCommunity Patient Education Preparation Projectapi-272791065Ainda não há avaliações
- Kuliah Periodic Paralysis Akibat TirotoksikosisDocumento14 páginasKuliah Periodic Paralysis Akibat TirotoksikosisFarnida JamhalAinda não há avaliações
- Perineural Versus Intravenous Dexamethasone As An Adjuvant For Peripheral Nerve BlocksDocumento8 páginasPerineural Versus Intravenous Dexamethasone As An Adjuvant For Peripheral Nerve Blockssome buddyyAinda não há avaliações
- Last Exams Questions Papers 2018 Dr. Gopika PDFDocumento111 páginasLast Exams Questions Papers 2018 Dr. Gopika PDFrhea100% (1)
- MECHANICAL DISORDERS OF SWALLOWING - PDF / KUNNAMPALLIL GEJODocumento91 páginasMECHANICAL DISORDERS OF SWALLOWING - PDF / KUNNAMPALLIL GEJOKUNNAMPALLIL GEJO JOHNAinda não há avaliações
- The Abdominojugular Reflux Sign: Jeff Wiese, MDDocumento3 páginasThe Abdominojugular Reflux Sign: Jeff Wiese, MDRed RubyAinda não há avaliações
- Pathogenesis of Pleural EffusionDocumento1 páginaPathogenesis of Pleural EffusionKlean Jee Teo-TrazoAinda não há avaliações
- AnxietyDocumento2 páginasAnxietyikoiAinda não há avaliações
- Normal Lab Values For PediatricsDocumento15 páginasNormal Lab Values For PediatricsJE MagbanuaAinda não há avaliações
- Putting BOTOX Facial Fillers Into PracticeDocumento62 páginasPutting BOTOX Facial Fillers Into PracticeVinisha Vipin Sharma100% (8)
- New Microsoft Office Word DocumentDocumento11 páginasNew Microsoft Office Word DocumentMihaela AndreiAinda não há avaliações
- Therapeutic Guidelines Antimicrobial Prophylaxis SurgeryDocumento86 páginasTherapeutic Guidelines Antimicrobial Prophylaxis SurgeryhendryfransiskusAinda não há avaliações
- WCECS2015 pp297-301Documento299 páginasWCECS2015 pp297-301Sivakumar RajarathinamAinda não há avaliações
- MRI MAGNETOM Avanto Upgradebrochure 152074006 7Documento56 páginasMRI MAGNETOM Avanto Upgradebrochure 152074006 7medjed1Ainda não há avaliações
- Ebn FormatDocumento5 páginasEbn FormatAngelica Mae ArenzanaAinda não há avaliações
- Nursing Exam Questions 2023 Part 8Documento3 páginasNursing Exam Questions 2023 Part 8Lejo SunnyAinda não há avaliações
- Temp Flex RPDDocumento4 páginasTemp Flex RPDAdam PhillipsAinda não há avaliações
- Anesthesia OverviewDocumento6 páginasAnesthesia OverviewAlan RoqueAinda não há avaliações
- User Manual: SoleolineDocumento104 páginasUser Manual: SoleolineERIKAinda não há avaliações