Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- RBG - CRM BRD - Marketing - v4.1Documento68 páginasRBG - CRM BRD - Marketing - v4.1Manvi Pareek100% (2)
- Engineering ConsultancyDocumento30 páginasEngineering Consultancynaconnet100% (2)
- Precision Nutrition. Nutrient TimingDocumento21 páginasPrecision Nutrition. Nutrient TimingPaolo AltoéAinda não há avaliações
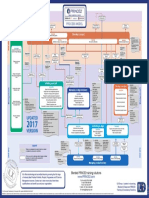
- p2 Process Model 2017Documento1 páginap2 Process Model 2017Miguel Fernandes0% (1)
- Heirs of Candelaria V RomeroDocumento2 páginasHeirs of Candelaria V Romeromoniquehadjirul100% (1)
- Antennas and Wave Propagation: Subject Code: Regulations: R16 JNTUH Class:III Year B.Tech ECE II SemesterDocumento18 páginasAntennas and Wave Propagation: Subject Code: Regulations: R16 JNTUH Class:III Year B.Tech ECE II SemesterSriAinda não há avaliações
- Spanish Web PDFDocumento36 páginasSpanish Web PDFSergio SayagoAinda não há avaliações
- Muzakarah Jawatankuasa Fatwa Majlis Kebangsaan Bagi Hal Ehwal Ugama Islam Malaysia Kali KeDocumento7 páginasMuzakarah Jawatankuasa Fatwa Majlis Kebangsaan Bagi Hal Ehwal Ugama Islam Malaysia Kali KeSiti Zubaidah ZulkhairieAinda não há avaliações
- Macguffin: History and UseDocumento5 páginasMacguffin: History and UseGeraldo CostaAinda não há avaliações
- The Scopes TrialDocumento10 páginasThe Scopes Trialapi-607238202Ainda não há avaliações
- Maintenance ManagerDocumento4 páginasMaintenance Managerapi-121382389Ainda não há avaliações
- HaDocumento15 páginasHaNicole Easther GabilangosoAinda não há avaliações
- LEC 2017 - Post-Test in Organized Crime InvesDocumento8 páginasLEC 2017 - Post-Test in Organized Crime InvesBokhary Dimasangkay Manok EliasAinda não há avaliações
- I. Revised Penal Code (RPC) and Related Special Laws: Riminal AWDocumento11 páginasI. Revised Penal Code (RPC) and Related Special Laws: Riminal AWMc Vharn CatreAinda não há avaliações
- YCAP 7 Steps PosterDocumento1 páginaYCAP 7 Steps PosterSohila AmrAinda não há avaliações
- Kosem SultanDocumento2 páginasKosem SultanAmaliaAinda não há avaliações
- John 20 Study GuideDocumento11 páginasJohn 20 Study GuideCongregation Shema YisraelAinda não há avaliações
- Law of Conservation of MassDocumento7 páginasLaw of Conservation of Massحمائل سجادAinda não há avaliações
- Audio Scripts B1 Student'S Book: CD 4 Track 38Documento2 páginasAudio Scripts B1 Student'S Book: CD 4 Track 38Priscila De La Rosa0% (1)
- Unit 9:: What Did You See at The Zoo?Documento11 páginasUnit 9:: What Did You See at The Zoo?ARiFin MoHaMedAinda não há avaliações
- 9702 s02 QP 1Documento20 páginas9702 s02 QP 1Yani AhmadAinda não há avaliações
- Not PrecedentialDocumento5 páginasNot PrecedentialScribd Government DocsAinda não há avaliações
- TENSES ExerciseDocumento28 páginasTENSES ExerciseKhanh PhamAinda não há avaliações
- The Effectiveness of Peppermint Oil (Mentha X Pepipirita) As Mosquito RepellentDocumento4 páginasThe Effectiveness of Peppermint Oil (Mentha X Pepipirita) As Mosquito RepellentKester PlaydaAinda não há avaliações
- SATB All Glory Laud and HonorDocumento1 páginaSATB All Glory Laud and HonorGeorge Orillo BaclayAinda não há avaliações
- MATH3161 MATH5165 T1 2023 OutlineDocumento10 páginasMATH3161 MATH5165 T1 2023 OutlineDouglusAinda não há avaliações
- Meralco v. CastilloDocumento2 páginasMeralco v. CastilloJoven CamusAinda não há avaliações
- 10 Applications in Engineering Mechanics PDFDocumento10 páginas10 Applications in Engineering Mechanics PDFWolf Lord100% (1)
- Chapter 15 NegotiationsDocumento16 páginasChapter 15 NegotiationsAdil HayatAinda não há avaliações
- Attitudes and Attitude ChangeDocumento19 páginasAttitudes and Attitude Changeprajwal-athrey-3069Ainda não há avaliações