Você também pode gostar
- (Kasus-Endokrin) (2016!11!10) A Management of Type 2 Diabetes Mellitus and Hyperglycemic Hyperosmolar State in A Patient With Pulmonary Tuberculosis (Ismayadi)Documento11 páginas(Kasus-Endokrin) (2016!11!10) A Management of Type 2 Diabetes Mellitus and Hyperglycemic Hyperosmolar State in A Patient With Pulmonary Tuberculosis (Ismayadi)Fariz NurAinda não há avaliações
- Fatal Leptopsirosis CaseDocumento6 páginasFatal Leptopsirosis CaseFariz NurAinda não há avaliações
- Antinuclear Antibodies: When To Test and How To Interpret FindingsDocumento4 páginasAntinuclear Antibodies: When To Test and How To Interpret FindingsFariz NurAinda não há avaliações
- 2015 AHA Guidelines Highlights EnglishDocumento36 páginas2015 AHA Guidelines Highlights EnglishshiloinAinda não há avaliações
- Ana TestDocumento4 páginasAna TestFariz NurAinda não há avaliações
- Pathophysiology of AKI BasileDocumento99 páginasPathophysiology of AKI BasileFariz NurAinda não há avaliações
- Guidelines For The Prevention, Care And... Ic Hepatitis B PDFDocumento16 páginasGuidelines For The Prevention, Care And... Ic Hepatitis B PDFFariz NurAinda não há avaliações
- Respiratory Tract InfectionDocumento13 páginasRespiratory Tract InfectionFariz NurAinda não há avaliações
- Di, Siadh, CSWDocumento17 páginasDi, Siadh, CSWVanitha Ratha KrishnanAinda não há avaliações
- Respiratory Tract InfectionDocumento13 páginasRespiratory Tract InfectionFariz NurAinda não há avaliações
- En Wikipedia Org Wiki Absolute Neutrophil CountDocumento5 páginasEn Wikipedia Org Wiki Absolute Neutrophil CountFariz NurAinda não há avaliações
- Frailty, John E. MorleyDocumento11 páginasFrailty, John E. MorleyFariz NurAinda não há avaliações
- Ethionamide-Induced Hypothyroidism in ChildrenDocumento3 páginasEthionamide-Induced Hypothyroidism in ChildrenFariz NurAinda não há avaliações
- Di, Siadh, CSWDocumento17 páginasDi, Siadh, CSWVanitha Ratha KrishnanAinda não há avaliações
- Insiden RematologiDocumento11 páginasInsiden RematologiFariz NurAinda não há avaliações
- Steroid Lupus NefritisDocumento3 páginasSteroid Lupus NefritisFariz NurAinda não há avaliações
- En Wikipedia Org Wiki Absolute Neutrophil CountDocumento5 páginasEn Wikipedia Org Wiki Absolute Neutrophil CountFariz NurAinda não há avaliações
- Ethionamide-Induced Hypothyroidism in ChildrenDocumento3 páginasEthionamide-Induced Hypothyroidism in ChildrenFariz NurAinda não há avaliações
- Neutrophil GranulocyteDocumento16 páginasNeutrophil GranulocyteFariz NurAinda não há avaliações
- Understanding The Epidemiology SleDocumento12 páginasUnderstanding The Epidemiology SleFariz NurAinda não há avaliações
- Helicobacter Pylori Eradication: Changes in Gastric Acid Secretion Assayed by Endoscopic Gastrin Test Before and AfterDocumento7 páginasHelicobacter Pylori Eradication: Changes in Gastric Acid Secretion Assayed by Endoscopic Gastrin Test Before and AfterFariz NurAinda não há avaliações
- H.pylori Dan CA GasterDocumento32 páginasH.pylori Dan CA GasterFariz NurAinda não há avaliações
- Gut 1998 Shimoyama S2 5 - 2Documento5 páginasGut 1998 Shimoyama S2 5 - 2Fariz NurAinda não há avaliações
- Ptre HT and MortalitasDocumento15 páginasPtre HT and MortalitasFariz NurAinda não há avaliações
- Factors Associated With ParadoxicalDocumento11 páginasFactors Associated With ParadoxicalFariz NurAinda não há avaliações
- Ajg 1998292 ADocumento9 páginasAjg 1998292 AFariz NurAinda não há avaliações
- Death Fariz 2-1-14Documento5 páginasDeath Fariz 2-1-14Fariz NurAinda não há avaliações
- Hyperbaric Oxygen Therapy: ReferenceDocumento5 páginasHyperbaric Oxygen Therapy: ReferenceFariz NurAinda não há avaliações
- Hyperbaric Oxygen Therapy: ReferenceDocumento5 páginasHyperbaric Oxygen Therapy: ReferenceFariz NurAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Gsis V RaoetDocumento1 páginaGsis V RaoetRekaire YantoAinda não há avaliações
- IVHDocumento2 páginasIVHHendra Boy SitumorangAinda não há avaliações
- Case Presentation: Dengue Hemorrhagic Fever Presented By: Vernalin B. TerradoDocumento55 páginasCase Presentation: Dengue Hemorrhagic Fever Presented By: Vernalin B. TerradoMaria Theszha AAinda não há avaliações
- First Aid:: Bleedin GDocumento20 páginasFirst Aid:: Bleedin GVielka Adap100% (1)
- Haamid2017 PDFDocumento25 páginasHaamid2017 PDFAhmad SyaukatAinda não há avaliações
- Blood and Cell Physiology MCQs With KeyDocumento9 páginasBlood and Cell Physiology MCQs With KeyMudassar Roomi88% (64)
- Ananya Deb - 18IUT0290004Documento26 páginasAnanya Deb - 18IUT0290004subankar NagAinda não há avaliações
- Complications of Bleeding Disorders in PregnancyDocumento11 páginasComplications of Bleeding Disorders in PregnancyNursing ReviewerAinda não há avaliações
- Trauma UretraDocumento3 páginasTrauma UretraTita FadiahAinda não há avaliações
- A New Understanding of The Coagulation ProcessDocumento6 páginasA New Understanding of The Coagulation Processwuryan dewiAinda não há avaliações
- Bio OneDocumento14 páginasBio OneLeeroyAinda não há avaliações
- Hematology 2 TEST QUESTIONSDocumento4 páginasHematology 2 TEST QUESTIONSa a r o n b a u t i s t aAinda não há avaliações
- Tranexamic AcidDocumento3 páginasTranexamic AcidEchik Rodriguez100% (2)
- Bleeding TimeDocumento47 páginasBleeding Timechickenbacon34Ainda não há avaliações
- Nursingcrib Com NURSING CARE PLAN Hepatitis ADocumento2 páginasNursingcrib Com NURSING CARE PLAN Hepatitis APravesh Verma100% (1)
- Foundations PDFDocumento10 páginasFoundations PDFmariasimbalAinda não há avaliações
- Blood & Blood ProductsDocumento126 páginasBlood & Blood ProductsdrprasadingleyAinda não há avaliações
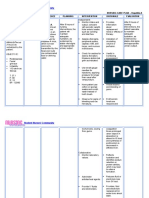
- Mod 3C Nursing Care Plan - Macanas, Evangeline Anne A. BSN 2BDocumento4 páginasMod 3C Nursing Care Plan - Macanas, Evangeline Anne A. BSN 2BEvangeline Anne MacanasAinda não há avaliações
- Amity Jaipur, Trial Advocacy, April 2024Documento23 páginasAmity Jaipur, Trial Advocacy, April 2024Anant VyasAinda não há avaliações
- Disorders of Coagulation and Fibrinolysis: Presented By: Toyco, Psyche Earl Monserrat Rojo, Kyzsa FranzDocumento58 páginasDisorders of Coagulation and Fibrinolysis: Presented By: Toyco, Psyche Earl Monserrat Rojo, Kyzsa FranzFearless AngelAinda não há avaliações
- ITLC Questions 2019Documento9 páginasITLC Questions 2019Neil ThomasAinda não há avaliações
- DHF NCP 2Documento1 páginaDHF NCP 2mavefigAinda não há avaliações
- Pathology - T&D - QP - 29140078Documento24 páginasPathology - T&D - QP - 29140078Prachi ChaturvediAinda não há avaliações
- Dorothy M. Adcock, MDDocumento4 páginasDorothy M. Adcock, MDพอ วิดAinda não há avaliações
- Plavix Clopidogrel Drug CardDocumento1 páginaPlavix Clopidogrel Drug CardSheri490100% (1)
- Traumatology Orthopaedic EXAMDocumento219 páginasTraumatology Orthopaedic EXAMElo GonçalvesAinda não há avaliações
- Types of BleedingDocumento43 páginasTypes of BleedingLiam Francis G. BasaloAinda não há avaliações
- Hemostatic Disorder in ChildrenDocumento4 páginasHemostatic Disorder in ChildrenodiliajessicanpviaAinda não há avaliações
- Platelet Count in Predicting Bleeding Complication After Elective Endoscopy in Children With Portal Hypertension and ThrombocytopeniaDocumento4 páginasPlatelet Count in Predicting Bleeding Complication After Elective Endoscopy in Children With Portal Hypertension and ThrombocytopeniaMasri YaniAinda não há avaliações
- Bleeding DisordersDocumento34 páginasBleeding Disordersbpt2Ainda não há avaliações