Você também pode gostar
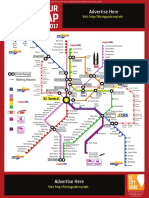
- Kuala Lumpur Train Map July 2017 LATESTDocumento3 páginasKuala Lumpur Train Map July 2017 LATESTvkhen88Ainda não há avaliações
- Jadwal DokterDocumento2 páginasJadwal Doktervkhen88Ainda não há avaliações
- Kuala Lumpur Train Map July 2017Documento1 páginaKuala Lumpur Train Map July 2017Mustafidzul MustaphaAinda não há avaliações
- PreventionDocumento3 páginasPreventionvkhen88Ainda não há avaliações
- CardioDocumento67 páginasCardiovkhen88Ainda não há avaliações
- Ws Ahf - Intro Apicd 2017 - EditedDocumento18 páginasWs Ahf - Intro Apicd 2017 - Editedvkhen88Ainda não há avaliações
- JournalDocumento16 páginasJournalvkhen88Ainda não há avaliações
- 2013 Stable Coronary Artery Disease Web AddendaDocumento32 páginas2013 Stable Coronary Artery Disease Web AddendaherbertglennyAinda não há avaliações
- 2015 ESC Pulmonary Hypertension (Guidelines On Diagnosis and Treatment Of)Documento58 páginas2015 ESC Pulmonary Hypertension (Guidelines On Diagnosis and Treatment Of)Muhammad Nur ArifinAinda não há avaliações
- Danareksa Management Trainee Application Form: Personal InformationDocumento1 páginaDanareksa Management Trainee Application Form: Personal InformationHerman HutabaratAinda não há avaliações
- Presentasi Kasus Kamis, 15 Januari 2015 Nama: Tn. M No. MR: 83-43-39 Umur: 55 Tahun Jenis Kelamin:Laki-laki Tanggal Perawatan: 6/12015Documento8 páginasPresentasi Kasus Kamis, 15 Januari 2015 Nama: Tn. M No. MR: 83-43-39 Umur: 55 Tahun Jenis Kelamin:Laki-laki Tanggal Perawatan: 6/12015vkhen88Ainda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (120)
- Cerebrovascular Accident (CVA) : The BrainDocumento6 páginasCerebrovascular Accident (CVA) : The BrainBrenn Marie RamosAinda não há avaliações
- Fondaparinux Guidelines 1Documento2 páginasFondaparinux Guidelines 1Tri Purma SariAinda não há avaliações
- Dr. Brendalyn A. Gallebo Department of Histopath and LaboratoriesDocumento216 páginasDr. Brendalyn A. Gallebo Department of Histopath and LaboratoriesFelyne Angelique C. GanoticeAinda não há avaliações
- Acls LectureDocumento15 páginasAcls LectureVincent BautistaAinda não há avaliações
- FibrinolysisDocumento26 páginasFibrinolysisCristinaGheorgheAinda não há avaliações
- Peripheral Vascular Disease Arteries NHSDocumento10 páginasPeripheral Vascular Disease Arteries NHSAdahl HetheringtonAinda não há avaliações
- Laboratory Evaluation FibrinolysisDocumento4 páginasLaboratory Evaluation FibrinolysisMaritoni ReyesAinda não há avaliações
- Heparin Induced ThrombocytopeniaDocumento17 páginasHeparin Induced ThrombocytopeniaTafsir arefin100% (1)
- Clinical Manifestations and Complications of Inflammatory Bowel Disease in Children and AdolescentsDocumento926 páginasClinical Manifestations and Complications of Inflammatory Bowel Disease in Children and AdolescentsFlorin Calin LungAinda não há avaliações
- Nursing Process MCQsDocumento8 páginasNursing Process MCQsedward osae-oppong86% (22)
- Manajemen StrokeDocumento253 páginasManajemen StrokeHappy Pramanda100% (2)
- Clinical Features and Diagnosis of Abdominal Aortic Aneurysm - UpToDateDocumento53 páginasClinical Features and Diagnosis of Abdominal Aortic Aneurysm - UpToDateALVARO ARIASAinda não há avaliações
- Tourniquet in Surgery of The Limbs: A Review of History, Types and ComplicationsDocumento6 páginasTourniquet in Surgery of The Limbs: A Review of History, Types and ComplicationsPatton SnowAinda não há avaliações
- Venous Supply of Head, Neck and FaceDocumento67 páginasVenous Supply of Head, Neck and FaceAlisha AranhaAinda não há avaliações
- ECMO For COVID 19 Updated 2021 Guidelines From.98326Documento42 páginasECMO For COVID 19 Updated 2021 Guidelines From.98326risanataliasiburianAinda não há avaliações
- Vitamin E Book For Ailing and Healthy Hearts - Wilfrid Shute PDF (Orthomolecular Medicine)Documento212 páginasVitamin E Book For Ailing and Healthy Hearts - Wilfrid Shute PDF (Orthomolecular Medicine)Anonymous gwFqQcnaX80% (5)
- ThrombophlebitisDocumento3 páginasThrombophlebitismirrejAinda não há avaliações
- Emergency Management of Pulmonary EmbolismsDocumento14 páginasEmergency Management of Pulmonary EmbolismsAmit RamrattanAinda não há avaliações
- DsaDocumento235 páginasDsaLalaine De Jesus100% (1)
- Nephrotic Syndrome-1Documento21 páginasNephrotic Syndrome-1Wondimu EliasAinda não há avaliações
- CoagulopathyDocumento121 páginasCoagulopathyMegat Mohd Azman AdzmiAinda não há avaliações
- Physical Therapy ReviewDocumento4 páginasPhysical Therapy Reviewpearl042008100% (1)
- The Society For Vascular Surgery Clinical Practice Guidelines On Popliteal Artery AneurysmsDocumento12 páginasThe Society For Vascular Surgery Clinical Practice Guidelines On Popliteal Artery AneurysmsGhaithAinda não há avaliações
- CUVASLARDocumento21 páginasCUVASLARKristal MartinezAinda não há avaliações
- Memorize BiologyDocumento79 páginasMemorize BiologyprthrAinda não há avaliações
- Chapter 026 CoagulationDocumento7 páginasChapter 026 Coagulationthubtendrolma100% (3)
- Guideline Trombositosis 2004Documento18 páginasGuideline Trombositosis 2004Jicko Street HooligansAinda não há avaliações
- Hematology 2 SummaryDocumento8 páginasHematology 2 Summarymonzon.mika1801Ainda não há avaliações
- CvaDocumento20 páginasCvanuraAinda não há avaliações