Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- Steroids PDFDocumento35 páginasSteroids PDFPratyusha VallamAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Pink Panther - Diabetes Management - Chapter 25Documento6 páginasPink Panther - Diabetes Management - Chapter 25jennmoyerAinda não há avaliações
- Pink Panther - Diabetes Management - Chapter 14Documento10 páginasPink Panther - Diabetes Management - Chapter 14jennmoyerAinda não há avaliações
- Pink Panther - Diabetes Management - Chapter 18Documento10 páginasPink Panther - Diabetes Management - Chapter 18jennmoyerAinda não há avaliações
- Pink Panther - Diabetes Management - Chapter 15Documento10 páginasPink Panther - Diabetes Management - Chapter 15jennmoyerAinda não há avaliações
- Pink Panther - Diabetes Management - Chapter 1Documento6 páginasPink Panther - Diabetes Management - Chapter 1jennmoyerAinda não há avaliações
- Pink Panther - Diabetes Management - Chapter 28Documento8 páginasPink Panther - Diabetes Management - Chapter 28jennmoyerAinda não há avaliações
- Chapter 09: Photo Atlas of Drug Administration Test Bank: Multiple ChoiceDocumento8 páginasChapter 09: Photo Atlas of Drug Administration Test Bank: Multiple ChoicePrettygirl716Ainda não há avaliações
- Pink Panther - Diabetes Management - Chapter 16Documento12 páginasPink Panther - Diabetes Management - Chapter 16jennmoyerAinda não há avaliações
- Pink Panther - Diabetes Management - Chapter 26Documento22 páginasPink Panther - Diabetes Management - Chapter 26jennmoyer100% (1)
- Pink Panther - Diabetes Management - Chapter 22Documento16 páginasPink Panther - Diabetes Management - Chapter 22jennmoyerAinda não há avaliações
- Pink Panther - Diabetes Management - Chapter 24Documento4 páginasPink Panther - Diabetes Management - Chapter 24jennmoyerAinda não há avaliações
- Pink Panther - Diabetes Management - Chapter 29Documento11 páginasPink Panther - Diabetes Management - Chapter 29jennmoyerAinda não há avaliações
- Pink Panther - Diabetes Management - Chapter 5Documento6 páginasPink Panther - Diabetes Management - Chapter 5jennmoyerAinda não há avaliações
- Pink Panther - Diabetes Management - Chapter 13Documento16 páginasPink Panther - Diabetes Management - Chapter 13jennmoyerAinda não há avaliações
- Pink Panther - Diabetes Management - Chapter 7Documento16 páginasPink Panther - Diabetes Management - Chapter 7jennmoyerAinda não há avaliações
- Pink Panther - Diabetes Management - Chapter 11Documento18 páginasPink Panther - Diabetes Management - Chapter 11jennmoyerAinda não há avaliações
- Pink Panther - Diabetes Management - Chapter 23Documento18 páginasPink Panther - Diabetes Management - Chapter 23jennmoyerAinda não há avaliações
- Pink Panther - Diabetes Management - Chapter 12Documento22 páginasPink Panther - Diabetes Management - Chapter 12jennmoyer100% (1)
- Pink Panther - Diabetes Management - Chapter 21Documento14 páginasPink Panther - Diabetes Management - Chapter 21jennmoyerAinda não há avaliações
- Pink Panther - Diabetes Management - Chapter 19Documento12 páginasPink Panther - Diabetes Management - Chapter 19jennmoyerAinda não há avaliações
- Pink Panther - Diabetes Management - Chapter 6Documento14 páginasPink Panther - Diabetes Management - Chapter 6jennmoyer100% (2)
- Pink Panther - Diabetes Management - Chapter 4Documento8 páginasPink Panther - Diabetes Management - Chapter 4jennmoyerAinda não há avaliações
- Pink Panther - Diabetes Management - Chapter 9Documento16 páginasPink Panther - Diabetes Management - Chapter 9jennmoyerAinda não há avaliações
- Pink Panther - Diabetes Management - Chapter 17Documento8 páginasPink Panther - Diabetes Management - Chapter 17jennmoyerAinda não há avaliações
- Pink Panther - Diabetes Management - Chapter 3Documento6 páginasPink Panther - Diabetes Management - Chapter 3jennmoyerAinda não há avaliações
- Feelings and Diabetes: Psychosocial AdjustmentDocumento4 páginasFeelings and Diabetes: Psychosocial AdjustmentjennmoyerAinda não há avaliações
- Understanding DiabetesDocumento6 páginasUnderstanding DiabetesjennmoyerAinda não há avaliações
- Drug InteractionDocumento60 páginasDrug InteractionAnkit GuptaAinda não há avaliações
- Insulin: T Ypes and Activit yDocumento0 páginaInsulin: T Ypes and Activit yClara DohudeAinda não há avaliações
- Rights and Tips Il StudentsDocumento2 páginasRights and Tips Il StudentsjennmoyerAinda não há avaliações
- Daily Log For DiabetesDocumento2 páginasDaily Log For DiabetesjennmoyerAinda não há avaliações
- Case StudyDocumento9 páginasCase Studyharshe vAinda não há avaliações
- The Evolution of Taiwan's National Health Insurance Drug Reimbursement SchemeDocumento7 páginasThe Evolution of Taiwan's National Health Insurance Drug Reimbursement Schemedewi assyah raniAinda não há avaliações
- Drug Discovery and Development: Understanding The R&D ProcessDocumento14 páginasDrug Discovery and Development: Understanding The R&D ProcessBandita DattaAinda não há avaliações
- Stock Opname Depo OkDocumento201 páginasStock Opname Depo Okidanursiani124Ainda não há avaliações
- DRUG STUDYDocumento2 páginasDRUG STUDYLarr SumalpongAinda não há avaliações
- LIST OF REGISTERED DRUGS As of December 2012: DR No Generic Brand Strength Form CompanyDocumento19 páginasLIST OF REGISTERED DRUGS As of December 2012: DR No Generic Brand Strength Form CompanyBenjamin TantiansuAinda não há avaliações
- ACTIV-6 Ivermectin One Pager 22NOV2021 0021Documento1 páginaACTIV-6 Ivermectin One Pager 22NOV2021 0021ABC Action NewsAinda não há avaliações
- Cannabis - The Original MedicineDocumento12 páginasCannabis - The Original MedicineAline PedrosoAinda não há avaliações
- Naloxone Flow Chart 3doses PDFDocumento1 páginaNaloxone Flow Chart 3doses PDFjoyceAinda não há avaliações
- Endo BagDocumento6 páginasEndo BagMarius NenciuAinda não há avaliações
- Lesson 2 Pharmacist Role in HTADocumento6 páginasLesson 2 Pharmacist Role in HTAJewell M. LicupAinda não há avaliações
- Praktikum Pengendalian IIDocumento22 páginasPraktikum Pengendalian IItrisna kurniaAinda não há avaliações
- 01 IntroductionDocumento45 páginas01 IntroductionTulin QadriAinda não há avaliações
- Nandani Product ListDocumento8 páginasNandani Product ListbilletonAinda não há avaliações
- IV To PO Conversion PolicyDocumento4 páginasIV To PO Conversion PolicyIrham NiAinda não há avaliações
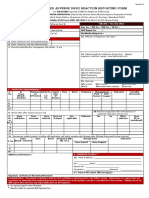
- ADRnewReporting Form 1.4Documento2 páginasADRnewReporting Form 1.4Sourabh kundara0% (1)
- Cheat Sheet Study Guide For ClinicalDocumento3 páginasCheat Sheet Study Guide For ClinicalXiomara GarciaAinda não há avaliações
- Drug Dosage Forms II (PHR 312) Course OverviewDocumento12 páginasDrug Dosage Forms II (PHR 312) Course OverviewprinceamitAinda não há avaliações
- Calculations in Toxicology and Determination of Median Effective and Median Lethal DosesDocumento3 páginasCalculations in Toxicology and Determination of Median Effective and Median Lethal DosesHammad KingAinda não há avaliações
- Unit 7. Sympathomimetics and SympatholyticsDocumento44 páginasUnit 7. Sympathomimetics and SympatholyticsApril Mergelle Lapuz100% (2)
- Deal 09 0123Documento48 páginasDeal 09 0123Zefa FanyaAinda não há avaliações
- Section 2.0 Active Ingredients: (S) - MethopreneDocumento71 páginasSection 2.0 Active Ingredients: (S) - Methopreneakhilkhattar1Ainda não há avaliações
- Which Drugs Can Cause Neuroleptic Malignant Syndrome?: Medicines Q&AsDocumento6 páginasWhich Drugs Can Cause Neuroleptic Malignant Syndrome?: Medicines Q&AsLaily MasrurohAinda não há avaliações
- TETANUS ANTITOXIN (EQUINE) - MSF Medical GuidelinesDocumento2 páginasTETANUS ANTITOXIN (EQUINE) - MSF Medical GuidelinesDanielAinda não há avaliações
- Synthetic MarijuanaDocumento4 páginasSynthetic MarijuanaZach SmithAinda não há avaliações
- Overview of Total Intravenous Anesthesia in ChildrenDocumento12 páginasOverview of Total Intravenous Anesthesia in ChildrenJosibel OcantoAinda não há avaliações
- Apotek AlfazzaDocumento32 páginasApotek Alfazzajihan.luthfiyahAinda não há avaliações