Você também pode gostar
- Case StudyDocumento11 páginasCase Studyapi-507420243100% (1)
- Pragyan College of Nursing Bhopal, M.P.: Subject - Mental Health Nursing TopicDocumento11 páginasPragyan College of Nursing Bhopal, M.P.: Subject - Mental Health Nursing Topicannu100% (1)
- Mental Health Case StudyDocumento11 páginasMental Health Case Studyapi-453449063Ainda não há avaliações
- Case 2Documento8 páginasCase 2Kreshnik IdrizajAinda não há avaliações
- Case Presentation - 1Documento19 páginasCase Presentation - 1GERA SUMANTHAinda não há avaliações
- Schizphrenia Nursing Car PlanDocumento2 páginasSchizphrenia Nursing Car PlanAmjad AliAinda não há avaliações
- Nursing Care Plan For Schizophrenic PatientsDocumento6 páginasNursing Care Plan For Schizophrenic PatientsHARVEY SELIMAinda não há avaliações
- Process RecordingDocumento4 páginasProcess RecordingSheena MosesAinda não há avaliações
- Process Recording 2Documento7 páginasProcess Recording 2Hardeep KaurAinda não há avaliações
- Psychiatry Case StudyDocumento21 páginasPsychiatry Case StudyJimmy MainaAinda não há avaliações
- Mrs. Sunanda's History and Mental Status Exam for DepressionDocumento12 páginasMrs. Sunanda's History and Mental Status Exam for DepressionamitAinda não há avaliações
- Nursing Care Plan Dissociative... 2 JanDocumento18 páginasNursing Care Plan Dissociative... 2 Janannu100% (1)
- A Case of DepressionDocumento11 páginasA Case of DepressionKabilan R100% (1)
- Process Recording: I Demographic DataDocumento27 páginasProcess Recording: I Demographic DataKavita kumari100% (2)
- Balbir Singh CPDocumento31 páginasBalbir Singh CPAyushiAinda não há avaliações
- MHN, I (U), 6Documento51 páginasMHN, I (U), 6akilaAinda não há avaliações
- Annotated BibliographyDocumento4 páginasAnnotated Bibliographymerin sunilAinda não há avaliações
- 2.A Ndera CaseDocumento14 páginas2.A Ndera CaseNsengimana Eric MaxigyAinda não há avaliações
- Drugs (Chino&anna)Documento15 páginasDrugs (Chino&anna)Nic JiAinda não há avaliações
- Bipolar Affective Disorder, Manic Episode With PsychoticDocumento30 páginasBipolar Affective Disorder, Manic Episode With PsychoticCharan Pal SinghAinda não há avaliações
- CASE PRESENTATION PP - Anxiety. Tiffany GordonDocumento6 páginasCASE PRESENTATION PP - Anxiety. Tiffany GordonTiffany GordonAinda não há avaliações
- Ocd MseDocumento8 páginasOcd MseGogs Ediza AlejoAinda não há avaliações
- Rle AssDocumento5 páginasRle AssMikaCasimiroBalunanAinda não há avaliações
- Mental Retardation Treatment and ManagementDocumento12 páginasMental Retardation Treatment and ManagementMelchoniza CalagoAinda não há avaliações
- Bipolar NCPDocumento2 páginasBipolar NCPAngel BunolAinda não há avaliações
- Mental Status Examination (MSE)Documento13 páginasMental Status Examination (MSE)Pia Mae Buaya100% (1)
- Alcoholism Care PlanDocumento11 páginasAlcoholism Care Planilakkiya ilakkiyaAinda não há avaliações
- The Psychiatric Mental Status Exam (MSE)Documento4 páginasThe Psychiatric Mental Status Exam (MSE)dev100% (1)
- Ocd First 3 PageDocumento5 páginasOcd First 3 Pagevikas takAinda não há avaliações
- Mental Status Examination: Identification DataDocumento5 páginasMental Status Examination: Identification Datailakkiya ilakkiyaAinda não há avaliações
- CHN Case Pres No Course in The Ward New 2 1 EmeDocumento33 páginasCHN Case Pres No Course in The Ward New 2 1 EmeJediah Rei TangonanAinda não há avaliações
- I. General ObjectiveDocumento5 páginasI. General ObjectiveMr. BQAinda não há avaliações
- Comprehensive Study of Paranoid Schizophrenia: Submitted byDocumento39 páginasComprehensive Study of Paranoid Schizophrenia: Submitted byPatricia Lingad RNAinda não há avaliações
- Mieliu TherapyDocumento7 páginasMieliu TherapyRENJULALAinda não há avaliações
- Causes and Treatment of ManiaDocumento11 páginasCauses and Treatment of ManiaGEETA MOHAN100% (2)
- Ihbas ReportDocumento11 páginasIhbas ReportSeema YadavAinda não há avaliações
- Psy CP FDocumento24 páginasPsy CP FShreya SinhaAinda não há avaliações
- Gracious College of Nursing Abhanpur Raipur (C.G.) : SubjectDocumento22 páginasGracious College of Nursing Abhanpur Raipur (C.G.) : SubjectMr. Psycho SamAinda não há avaliações
- Process Recording, Suicide Assesment and Psyche-Med ConditionDocumento44 páginasProcess Recording, Suicide Assesment and Psyche-Med ConditionShy Dela PuertaAinda não há avaliações
- Hiatal HerniaDocumento3 páginasHiatal HerniaJobelle AcenaAinda não há avaliações
- Psy Case StudyDocumento81 páginasPsy Case StudyIOM BNSAinda não há avaliações
- Seminar 7Documento27 páginasSeminar 7Arya Lekshmi100% (1)
- Case StudyDocumento13 páginasCase StudyJimmy MainaAinda não há avaliações
- Depression Case StudyDocumento1 páginaDepression Case StudyNicole cuencos100% (1)
- Case StudyDocumento17 páginasCase Studyapi-508597583Ainda não há avaliações
- Lesson Plan BlankDocumento41 páginasLesson Plan Blankindhu100% (1)
- Milieu Therapy: An Interdisciplinary ApproachDocumento17 páginasMilieu Therapy: An Interdisciplinary ApproachAntro BerrinAinda não há avaliações
- Milieu TherapyDocumento4 páginasMilieu TherapyManu Sethi100% (1)
- MMSE1Documento4 páginasMMSE1nikithaa saravananAinda não há avaliações
- Organic Mental Disorder: Presented By: Priyanka Kumari M.Sc. NursingDocumento50 páginasOrganic Mental Disorder: Presented By: Priyanka Kumari M.Sc. NursingHardeep KaurAinda não há avaliações
- Misconception About Mental Illness213054872 PDFDocumento27 páginasMisconception About Mental Illness213054872 PDFyangi dokaAinda não há avaliações
- Care Plan 9 Substance Use DisorderDocumento18 páginasCare Plan 9 Substance Use DisorderLokeshwari KatreAinda não há avaliações
- Nursing Process PsychiatricDocumento13 páginasNursing Process PsychiatricamitAinda não há avaliações
- Structured Format For History and MSEDocumento22 páginasStructured Format For History and MSEfizAinda não há avaliações
- Case StudyDocumento9 páginasCase StudyKavita KavAinda não há avaliações
- Mental Health Nursing Case StudyDocumento9 páginasMental Health Nursing Case Studyapi-454984300Ainda não há avaliações
- Postpartum Psychosis Case ScenarioDocumento2 páginasPostpartum Psychosis Case ScenarioEden CruzAinda não há avaliações
- Nursing Care Plan for Mental Retardation and SchizophreniaDocumento20 páginasNursing Care Plan for Mental Retardation and SchizophreniaSARITA SHARMAAinda não há avaliações
- Nursing Care Plan For A Patient With SchizophreniaDocumento14 páginasNursing Care Plan For A Patient With SchizophreniaBasma Elgharbawy100% (1)
- PDFDocumento64 páginasPDFJerilee SoCute WattsAinda não há avaliações
- SkinDocumento43 páginasSkinFhen Farrel100% (1)
- Digestive SystemDocumento48 páginasDigestive SystemJerilee SoCute WattsAinda não há avaliações
- The Circulatory System-: TransportDocumento13 páginasThe Circulatory System-: TransportJerilee SoCute WattsAinda não há avaliações
- The Digestive System EssayDocumento3 páginasThe Digestive System EssayJerilee SoCute Watts0% (1)
- The Digestive System Part 1Documento28 páginasThe Digestive System Part 1Jerilee SoCute WattsAinda não há avaliações
- Reproductive SystemDocumento80 páginasReproductive SystemJerilee SoCute WattsAinda não há avaliações
- Skin Diseases Disorders ConditionsDocumento104 páginasSkin Diseases Disorders ConditionsJerilee SoCute WattsAinda não há avaliações
- CV SYSTEM ANATOMYDocumento42 páginasCV SYSTEM ANATOMYJerilee SoCute WattsAinda não há avaliações
- Urinary SystemDocumento105 páginasUrinary SystemJerilee SoCute WattsAinda não há avaliações
- Respiratory System Anatomy and Functions EX36Documento57 páginasRespiratory System Anatomy and Functions EX36royanirudh99Ainda não há avaliações
- Reproduction and DevelopmentDocumento53 páginasReproduction and DevelopmentJerilee SoCute WattsAinda não há avaliações
- Digestive System: Stomach and Small Intestine FunctionsDocumento56 páginasDigestive System: Stomach and Small Intestine FunctionsJerilee SoCute WattsAinda não há avaliações
- The Conducting System of The HeartDocumento37 páginasThe Conducting System of The HeartJerilee SoCute WattsAinda não há avaliações
- The Lymphatic SystemDocumento50 páginasThe Lymphatic SystemJerilee SoCute Watts100% (1)
- Review Questions - Heart Anatomy & PhysiologyDocumento1 páginaReview Questions - Heart Anatomy & PhysiologyJerilee SoCute WattsAinda não há avaliações
- Respiratory System 1Documento29 páginasRespiratory System 1Jerilee SoCute WattsAinda não há avaliações
- Respiratory System 2Documento39 páginasRespiratory System 2Jerilee SoCute WattsAinda não há avaliações
- Lecture 21 - Respiratory SystemDocumento59 páginasLecture 21 - Respiratory SystemSkyBirdAinda não há avaliações
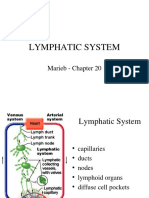
- Lymphatic System: Marieb Chapter 20Documento22 páginasLymphatic System: Marieb Chapter 20Jerilee SoCute WattsAinda não há avaliações
- Brain Respiratory Centers & Control MechanismsDocumento36 páginasBrain Respiratory Centers & Control MechanismsJerilee SoCute WattsAinda não há avaliações
- Reproductive System DisordersDocumento62 páginasReproductive System DisordersJerilee SoCute Watts100% (2)
- Human ReproductionDocumento42 páginasHuman ReproductionAliDarimiKRAinda não há avaliações
- Pulmonary and Systemic CircuitsDocumento38 páginasPulmonary and Systemic CircuitsJerilee SoCute WattsAinda não há avaliações
- Unit 6 OsmolarityDocumento59 páginasUnit 6 Osmolaritykrystal1994Ainda não há avaliações
- Lecture 1 Cardiovascular SystemDocumento70 páginasLecture 1 Cardiovascular SystemJerilee SoCute WattsAinda não há avaliações
- Reproduction Summary NotesDocumento16 páginasReproduction Summary NotesJerilee SoCute WattsAinda não há avaliações
- Reproduction NotesDocumento20 páginasReproduction NotesMario BaemamentengAinda não há avaliações
- Lecture 2 Cardiovascular SystemDocumento70 páginasLecture 2 Cardiovascular SystemJerilee SoCute WattsAinda não há avaliações
- Platelets and HemostasisDocumento19 páginasPlatelets and HemostasisJerilee SoCute WattsAinda não há avaliações
- Safe BuckDocumento2 páginasSafe BuckAnonymous rPV6LRE1Ainda não há avaliações
- Brooke Harris Lit Review 5Documento7 páginasBrooke Harris Lit Review 5api-548741189Ainda não há avaliações
- Instructional Design Documents - Funk EmilyDocumento25 páginasInstructional Design Documents - Funk Emilyapi-595583917Ainda não há avaliações
- Indira Gandhi National Tribal University, Amarkantak (M.P.) : Application Form For The Non-Teaching PostsDocumento4 páginasIndira Gandhi National Tribal University, Amarkantak (M.P.) : Application Form For The Non-Teaching PostssenomitaAinda não há avaliações
- TWI EssentialsDocumento1 páginaTWI Essentialssjaak0% (1)
- Least Mastered Skills With Graph Mean MTB MLEDocumento4 páginasLeast Mastered Skills With Graph Mean MTB MLEMA ASTERIA AGUSTINA CENALAinda não há avaliações
- GRE 9604 (6) NewDocumento18 páginasGRE 9604 (6) NewUsman KhalidAinda não há avaliações
- Coverletter Resume Thankyouletter - Taylor Cornwall-MooreDocumento4 páginasCoverletter Resume Thankyouletter - Taylor Cornwall-Mooreapi-578447660Ainda não há avaliações
- JIL Anniv - LGN AttendanceDocumento49 páginasJIL Anniv - LGN AttendanceMark TozukaAinda não há avaliações
- University of Engineering and Technology Lahore, PakistanDocumento2 páginasUniversity of Engineering and Technology Lahore, PakistanAsif HameedAinda não há avaliações
- Franco Around AbhinavaguptaDocumento25 páginasFranco Around AbhinavaguptaTyler Graham Neill100% (1)
- Community HealthDocumento23 páginasCommunity HealthGlizzle MacaraegAinda não há avaliações
- Justice Thesis StatementsDocumento5 páginasJustice Thesis StatementsLisa Garcia100% (2)
- Application 3 - Meghan PadialDocumento3 páginasApplication 3 - Meghan Padialapi-289849149Ainda não há avaliações
- OCC - Q1 - Module 9-Communicative strategies-EDITEDDocumento15 páginasOCC - Q1 - Module 9-Communicative strategies-EDITEDAMYTHEEZ CAMOMOT50% (2)
- Politics-IR UK 2014 WebDocumento36 páginasPolitics-IR UK 2014 Webnthu55660% (1)
- Handbook of TerminologyDocumento172 páginasHandbook of TerminologyAlina-Mihaela MikiAinda não há avaliações
- DIASS Q3 Module1Documento25 páginasDIASS Q3 Module1Gurleeyh VillsAinda não há avaliações
- Nambia: Annual Human Rights Report: 2008Documento252 páginasNambia: Annual Human Rights Report: 2008André Le RouxAinda não há avaliações
- Division of Cavite Trece Martirez City List of Private Secondary SchoolsDocumento115 páginasDivision of Cavite Trece Martirez City List of Private Secondary SchoolsEmely June Flores0% (1)
- Most Popular Chinese Tales With AnimalsDocumento64 páginasMost Popular Chinese Tales With AnimalsRita LeeAinda não há avaliações
- Seiwakai Newsletter Issue 54Documento13 páginasSeiwakai Newsletter Issue 54Laura FerreiraAinda não há avaliações
- General Grad ULAB Sum2013Documento9 páginasGeneral Grad ULAB Sum2013Baladi KushfusAinda não há avaliações
- Indian Community School - Kuwait Class XI Notes (2022-23): Making NotesDocumento5 páginasIndian Community School - Kuwait Class XI Notes (2022-23): Making NotesAnushka MishraAinda não há avaliações
- Volkswagen Balanced ScorecardDocumento1 páginaVolkswagen Balanced ScorecardFatima Medriza DuranAinda não há avaliações
- A Study On Working Women and Their InvestmentDocumento70 páginasA Study On Working Women and Their InvestmentRITIKA PATHAKAinda não há avaliações
- Interview Questions, Study Materials For Computer ScienceDocumento2 páginasInterview Questions, Study Materials For Computer ScienceInstitute of Engineering Studies (IES)Ainda não há avaliações
- Essay For MIL!Documento2 páginasEssay For MIL!Micha JugalbotAinda não há avaliações
- Philippine Christian University: The Problem and Its BackgroundDocumento30 páginasPhilippine Christian University: The Problem and Its BackgroundumbrellaAinda não há avaliações
- The Students Will AnswerDocumento8 páginasThe Students Will AnswerLexa Mae Quizon100% (2)