Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- (Kadar LDL Dan HDL Dalam Darah Model Tikus Periodontitis (Blood Level of LDL and HDL in Periodontitis Rat Model)Documento5 páginas(Kadar LDL Dan HDL Dalam Darah Model Tikus Periodontitis (Blood Level of LDL and HDL in Periodontitis Rat Model)Suma_DewiAinda não há avaliações
- DocumentDocumento9 páginasDocumentSuma_DewiAinda não há avaliações
- Free DocumentDocumento8 páginasFree DocumentSuma_DewiAinda não há avaliações
- ResearchDocumento11 páginasResearchSuma_DewiAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Kita Duktus TiroglosusDocumento5 páginasKita Duktus TiroglosusbarbiemeAinda não há avaliações
- BookchaptercraniofacialDocumento12 páginasBookchaptercraniofacialzeeshan bangashAinda não há avaliações
- Retention and RelapseDocumento92 páginasRetention and RelapseBimalKrishna100% (1)
- Brain CellsDocumento4 páginasBrain CellsJulius RicardeAinda não há avaliações
- Uji Reliabilitas Vertigo Symptom Scale Short Form VSS-SF Pada Penderita Dizziness Di RSUP Sanglah Denpasar PDFDocumento4 páginasUji Reliabilitas Vertigo Symptom Scale Short Form VSS-SF Pada Penderita Dizziness Di RSUP Sanglah Denpasar PDFyolan ariyanaAinda não há avaliações
- TNSS AU1.0 eng-AUori ReviewDocumento1 páginaTNSS AU1.0 eng-AUori ReviewRiany Jade SabrinaAinda não há avaliações
- Auditory TubeDocumento14 páginasAuditory TubeAbishek JAinda não há avaliações
- Shanz - Ent 1.07 NoseDocumento4 páginasShanz - Ent 1.07 NosePetrina XuAinda não há avaliações
- Bio 201 - Bone Practical Part 1 (Axial Skeleton)Documento5 páginasBio 201 - Bone Practical Part 1 (Axial Skeleton)Gretchen100% (1)
- Asymmetric Craniofacial AsymmetriesDocumento168 páginasAsymmetric Craniofacial AsymmetriessoujanyaAinda não há avaliações
- Children's Activity BookDocumento48 páginasChildren's Activity Bookojossaludables100% (3)
- Class. of Maxillectomy DefectsDocumento10 páginasClass. of Maxillectomy DefectsJASPREETKAUR0410Ainda não há avaliações
- NBDE Dental Boards Oral SurgeryDocumento30 páginasNBDE Dental Boards Oral SurgeryJoyce Lim100% (1)
- Isolated Abducens Nerve Palsy: Update On Evaluation and DiagnosisDocumento1 páginaIsolated Abducens Nerve Palsy: Update On Evaluation and DiagnosisalecsaAinda não há avaliações
- Race 2007 PDFDocumento236 páginasRace 2007 PDFRois Hasyim100% (1)
- Ent OsceDocumento15 páginasEnt OsceAntaraaAinda não há avaliações
- Less Than Total Thyroidectomy For Goiter When and HowDocumento10 páginasLess Than Total Thyroidectomy For Goiter When and HowTubagus NahnudinAinda não há avaliações
- Muscles of Mastication Sumana SeminarDocumento68 páginasMuscles of Mastication Sumana SeminarSumana AryaAinda não há avaliações
- Salivary GlandsDocumento97 páginasSalivary GlandsSwati George100% (2)
- Daftar Penyakit Telinga Hidung Tenggorok-Kepala Leher Menurut Icd 10Documento10 páginasDaftar Penyakit Telinga Hidung Tenggorok-Kepala Leher Menurut Icd 10kartianiAinda não há avaliações
- Essay Healthy Eyes and EarsDocumento8 páginasEssay Healthy Eyes and EarsMell Brigitte Cordova AlmonteAinda não há avaliações
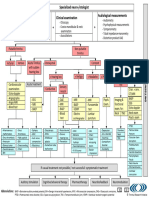
- TRI Tinnitus FlowchartDocumento1 páginaTRI Tinnitus FlowchartAdvocacia VitóriaAinda não há avaliações
- Patient Type: OPD: TSH Test ReportDocumento1 páginaPatient Type: OPD: TSH Test ReportVeenu SehrawatAinda não há avaliações
- Wiringtechniquesinmaxillofacialsurgery 121205104837 Phpapp01Documento41 páginasWiringtechniquesinmaxillofacialsurgery 121205104837 Phpapp01Dhini AnggrianiAinda não há avaliações
- Clinical Skills Cranial Nerves I To VI Students Copy 2019Documento4 páginasClinical Skills Cranial Nerves I To VI Students Copy 2019carlosAinda não há avaliações
- Disponibil in Pagina Cod DenumireDocumento3 páginasDisponibil in Pagina Cod DenumireSoryna IuliaAinda não há avaliações
- Headgear Appliances - Columbia New - BWDocumento8 páginasHeadgear Appliances - Columbia New - BWNana HindraAinda não há avaliações
- NEBDN Dental Charting Book APRIL 2015Documento13 páginasNEBDN Dental Charting Book APRIL 2015Avita RathAinda não há avaliações
- Ten Triangles Around Cavernous Sinus For Surgical Approach, Described by Schematic Diagram and Three Dimensional Models With The Sectioned ImagesDocumento9 páginasTen Triangles Around Cavernous Sinus For Surgical Approach, Described by Schematic Diagram and Three Dimensional Models With The Sectioned ImagesJesús Martín-FdezAinda não há avaliações
- ENT Toppers Scribble NotesDocumento5 páginasENT Toppers Scribble NotespvsvrAinda não há avaliações