Você também pode gostar
- Renin Angiotensin Aldosterone SystemDocumento1 páginaRenin Angiotensin Aldosterone Systemgdubs215Ainda não há avaliações
- Pericardium:: AnatomyDocumento4 páginasPericardium:: AnatomyAlya Putri KhairaniAinda não há avaliações
- RAASDocumento5 páginasRAASJamaica VillonAinda não há avaliações
- HypertensionDocumento5 páginasHypertensionCia Yee YeohAinda não há avaliações
- Kinesiology of Shoulder Complex MusclesDocumento7 páginasKinesiology of Shoulder Complex MusclesAlya Putri KhairaniAinda não há avaliações
- Manage Fluid Volume Excess in Renal FailureDocumento3 páginasManage Fluid Volume Excess in Renal FailureMichael Baylon DueñasAinda não há avaliações
- Pathology Polycystic Kidney DiseaseDocumento4 páginasPathology Polycystic Kidney DiseaseOnyedika EgbujoAinda não há avaliações
- Anal Canal: Fissure in Ano HaemorrhoidsDocumento37 páginasAnal Canal: Fissure in Ano Haemorrhoidsyash shrivastavaAinda não há avaliações
- Pathophysiology of Heart FailureDocumento2 páginasPathophysiology of Heart FailureJaysellePuguonTabijeAinda não há avaliações
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNo EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsAinda não há avaliações
- Stroke and Cerebrovascular DiseaseDocumento14 páginasStroke and Cerebrovascular DiseaseMarwan M.Ainda não há avaliações
- David Perlmutter Focus Autoimmune PDFDocumento23 páginasDavid Perlmutter Focus Autoimmune PDFutpal_thakar100% (6)
- Concept Map Worksheet Mary Richards Heart Failure Jasgou1752Documento3 páginasConcept Map Worksheet Mary Richards Heart Failure Jasgou1752Jasmyn Rose100% (1)
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- Glomerulonephritis 10Documento5 páginasGlomerulonephritis 10Eden Jay Calija AgoyAinda não há avaliações
- Hypertension Pathophysiology and Treatment PDFDocumento6 páginasHypertension Pathophysiology and Treatment PDFBella TogasAinda não há avaliações
- Hemodynamic MonitoringDocumento28 páginasHemodynamic MonitoringKimberlie Dela Merced Tomas100% (1)
- NAFLD - NASH and Present & Future Management OptionsDocumento78 páginasNAFLD - NASH and Present & Future Management OptionsSantosh AnandAinda não há avaliações
- Post-Streptococcal GlomerulonephritisDocumento18 páginasPost-Streptococcal GlomerulonephritisPreciousJemAinda não há avaliações
- Myocardialinfarction 150223043527 Conversion Gate02 PDFDocumento22 páginasMyocardialinfarction 150223043527 Conversion Gate02 PDFBhavika Aggarwal100% (1)
- Sickle Cell & ThalassemiaDocumento3 páginasSickle Cell & ThalassemiaJulia Rae Delos SantosAinda não há avaliações
- Rheumatic Fever: Causes, Tests, and Treatment OptionsNo EverandRheumatic Fever: Causes, Tests, and Treatment OptionsAinda não há avaliações
- Pathophysiology Diagram of Kawasaki Disease: Precipitating Factors: Predisposing FactorsDocumento2 páginasPathophysiology Diagram of Kawasaki Disease: Precipitating Factors: Predisposing FactorsAb Staholic Boii100% (1)
- Hanta Vi Ru S Inf Ection SDocumento20 páginasHanta Vi Ru S Inf Ection Stummalapalli venkateswara rao100% (3)
- Role of The Kidney in Long Term RegulationDocumento19 páginasRole of The Kidney in Long Term RegulationMelisa NovitasariAinda não há avaliações
- Heart FailureDocumento10 páginasHeart Failureurmila prajapatiAinda não há avaliações
- Pathophysiology MaiaDocumento2 páginasPathophysiology Maiajia88Ainda não há avaliações
- Idiopathic Thrombocytopenic Purpura (ITP)Documento7 páginasIdiopathic Thrombocytopenic Purpura (ITP)Rizqka PertiwiAinda não há avaliações
- Heart Valve DiseaseDocumento9 páginasHeart Valve DiseaseChaturangaNSenerathAinda não há avaliações
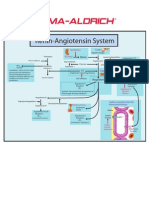
- Renin-Angiotensin SystemDocumento1 páginaRenin-Angiotensin SystemSigma-Aldrich100% (2)
- Nootropil: Qualitative and Quantitative CompositionDocumento12 páginasNootropil: Qualitative and Quantitative CompositionMuhammad TalhaAinda não há avaliações
- Causes and Symptoms of Beta-ThalassemiaDocumento1 páginaCauses and Symptoms of Beta-ThalassemiaAngie LamoAinda não há avaliações
- Rhabdomyolysis Case Study WeeblyDocumento18 páginasRhabdomyolysis Case Study Weeblyapi-241865788Ainda não há avaliações
- 1-Drugs Affecting Uterine Muscle ContractilityDocumento40 páginas1-Drugs Affecting Uterine Muscle ContractilityjojolilimomoAinda não há avaliações
- 2 Acute Myocardial InfarctionDocumento15 páginas2 Acute Myocardial InfarctionpauchanmnlAinda não há avaliações
- Glomerulonephritis vs GlomerulopathiesDocumento58 páginasGlomerulonephritis vs GlomerulopathiesRahmailla Khanza Diana FebriliantriAinda não há avaliações
- Idiopathic Thrombocytopenic Purpura: Overview With Report of A CaseDocumento4 páginasIdiopathic Thrombocytopenic Purpura: Overview With Report of A CaseHernan GonzalezAinda não há avaliações
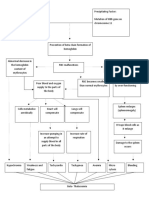
- Predisposing and precipitating factors leading to ESRD, DM, atherosclerosis, and pneumoniaDocumento11 páginasPredisposing and precipitating factors leading to ESRD, DM, atherosclerosis, and pneumoniaJonathan CuaAinda não há avaliações
- UtiDocumento38 páginasUtiAzra AzmunaAinda não há avaliações
- Burn Injury PathophysiologyDocumento1 páginaBurn Injury PathophysiologyMonique Ann DanoyAinda não há avaliações
- Schistosomiasis (From Anatomy To Pathophysiology)Documento10 páginasSchistosomiasis (From Anatomy To Pathophysiology)Tiger Knee100% (1)
- Pathophysiology of DiarrheaDocumento3 páginasPathophysiology of DiarrheaFathur RahmatAinda não há avaliações
- MIDocumento22 páginasMIGagauz SiliviaAinda não há avaliações
- Predisposing Conditions, Management and Prevention of Chronic Kidney DiseaseDocumento52 páginasPredisposing Conditions, Management and Prevention of Chronic Kidney DiseaseSaad MotawéaAinda não há avaliações
- Risk Factors and Types of LeukemiaDocumento3 páginasRisk Factors and Types of LeukemiaJulia Rae Delos SantosAinda não há avaliações
- Practice Teaching On Anemia: Presented By: Mr. Hari Singh Nagar M. SC Nursing 1 YearDocumento44 páginasPractice Teaching On Anemia: Presented By: Mr. Hari Singh Nagar M. SC Nursing 1 YearSundarAinda não há avaliações
- Cardiovascular LectureDocumento10 páginasCardiovascular LectureJaysonPangilinanAbanAinda não há avaliações
- Tetralogy of FallotDocumento38 páginasTetralogy of FallotJohn Paul MedalloAinda não há avaliações
- Pathophysiology of Rheumatic Heart Disease and FeverDocumento3 páginasPathophysiology of Rheumatic Heart Disease and FeverDee SarajanAinda não há avaliações
- 1 - Presentation - Management of Preclamplsia, Mild and ModerateDocumento22 páginas1 - Presentation - Management of Preclamplsia, Mild and ModeratesharonAinda não há avaliações
- TURP Procedure ExplainedDocumento36 páginasTURP Procedure ExplainedRight VentricleAinda não há avaliações
- Biomedical Case StudyDocumento5 páginasBiomedical Case StudyHannan AtharAinda não há avaliações
- Pharma - Drugs Affecting Git MotilityDocumento6 páginasPharma - Drugs Affecting Git MotilityBobet ReñaAinda não há avaliações
- Arterial Hypertension Eng PDFDocumento29 páginasArterial Hypertension Eng PDFagustinaw1981Ainda não há avaliações
- Case Study 2Documento4 páginasCase Study 2api-2451636590% (1)
- Bleeding DisordersDocumento24 páginasBleeding Disorderskholoud220Ainda não há avaliações
- 4.1agents For Hyperuricemia GoutDocumento4 páginas4.1agents For Hyperuricemia GoutjohntrueAinda não há avaliações
- Pamantasan NG Cabuyao College of Health Allied Sciences College of NursingDocumento43 páginasPamantasan NG Cabuyao College of Health Allied Sciences College of NursingSofea MustaffaAinda não há avaliações
- Nephrotic Syndrome PathophysiologyDocumento1 páginaNephrotic Syndrome PathophysiologyKrisianne Mae Lorenzo FranciscoAinda não há avaliações
- Endocrine SystemDocumento22 páginasEndocrine SystemLen Len Ochinang OchinangAinda não há avaliações
- Acute Myeloid Leukemia (Drug Study)Documento3 páginasAcute Myeloid Leukemia (Drug Study)Krisianne Mae Lorenzo FranciscoAinda não há avaliações
- Idiophatic Thrombocytopenic Purpura (ITP) in PregnancyDocumento27 páginasIdiophatic Thrombocytopenic Purpura (ITP) in PregnancyAdietya Bima PrakasaAinda não há avaliações
- Problem-based Approach to Gastroenterology and HepatologyNo EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisAinda não há avaliações
- Chapter 3 A Neuro Disorders Public H ChallengesDocumento71 páginasChapter 3 A Neuro Disorders Public H ChallengesAnna Francesca AbarquezAinda não há avaliações
- Renal Regulation of PotassiumDocumento5 páginasRenal Regulation of PotassiumAlya Putri KhairaniAinda não há avaliações
- Uric Acid and Its MetabolismDocumento3 páginasUric Acid and Its MetabolismAlya Putri KhairaniAinda não há avaliações
- Inhalation InjuryDocumento2 páginasInhalation InjuryAlya Putri KhairaniAinda não há avaliações
- Histogenesis and Cell Types in Bone FormationDocumento6 páginasHistogenesis and Cell Types in Bone FormationAlya Putri KhairaniAinda não há avaliações
- Inhalation InjuryDocumento2 páginasInhalation InjuryAlya Putri KhairaniAinda não há avaliações
- Community Nutrition & Physician's ResponsibilityDocumento16 páginasCommunity Nutrition & Physician's ResponsibilityAlya Putri KhairaniAinda não há avaliações
- Iccu / Cicu: Patients Heart Attacks Unstable Angina Cardiac DysrhythmiaDocumento4 páginasIccu / Cicu: Patients Heart Attacks Unstable Angina Cardiac DysrhythmiaAlya Putri KhairaniAinda não há avaliações
- Hypersensitivity Type IDocumento3 páginasHypersensitivity Type IAlya Putri KhairaniAinda não há avaliações
- Normal X RayDocumento6 páginasNormal X RayAlya Putri KhairaniAinda não há avaliações
- How Tetanus or Dental Caries Can Cause Cardiovascular DiseaseDocumento3 páginasHow Tetanus or Dental Caries Can Cause Cardiovascular DiseaseAlya Putri KhairaniAinda não há avaliações
- Bleeding: Blood VesselDocumento2 páginasBleeding: Blood VesselAlya Putri KhairaniAinda não há avaliações
- Leptospira SP.: Leptospira Are Spiral Bacteria (Spirochaete) in The Family of LeptospiraceaeDocumento3 páginasLeptospira SP.: Leptospira Are Spiral Bacteria (Spirochaete) in The Family of LeptospiraceaeAlya Putri KhairaniAinda não há avaliações
- Colorectal CacinomaDocumento2 páginasColorectal CacinomaAlya Putri KhairaniAinda não há avaliações
- Function of SinusesDocumento1 páginaFunction of SinusesAlya Putri KhairaniAinda não há avaliações
- Diagnosing and Managing Systemic Lupus ErythematosusDocumento3 páginasDiagnosing and Managing Systemic Lupus ErythematosusAlya Putri KhairaniAinda não há avaliações
- Failure To ThriveDocumento3 páginasFailure To ThriveAlya Putri KhairaniAinda não há avaliações
- Staging of HerniaDocumento1 páginaStaging of HerniaAlya Putri KhairaniAinda não há avaliações
- Colorectal CacinomaDocumento2 páginasColorectal CacinomaAlya Putri KhairaniAinda não há avaliações
- Anatomy of Oral RegionDocumento6 páginasAnatomy of Oral RegionAlya Putri KhairaniAinda não há avaliações
- Hemolytic Anemia: MorphologyDocumento10 páginasHemolytic Anemia: MorphologyAlya Putri KhairaniAinda não há avaliações
- Clobetasol Propionate and Urea CreamDocumento4 páginasClobetasol Propionate and Urea CreamAlya Putri KhairaniAinda não há avaliações
- Congenital Syphilis Causes and TreatmentDocumento4 páginasCongenital Syphilis Causes and TreatmentAlya Putri Khairani100% (1)
- Influenza: Laboratory FindingsDocumento6 páginasInfluenza: Laboratory FindingsAlya Putri KhairaniAinda não há avaliações
- Inhalation InjuryDocumento2 páginasInhalation InjuryAlya Putri KhairaniAinda não há avaliações
- Herpes VirusesDocumento6 páginasHerpes VirusesAlya Putri KhairaniAinda não há avaliações
- Leptospira SP.: Leptospira Are Spiral Bacteria (Spirochaete) in The Family of LeptospiraceaeDocumento3 páginasLeptospira SP.: Leptospira Are Spiral Bacteria (Spirochaete) in The Family of LeptospiraceaeAlya Putri KhairaniAinda não há avaliações
- Conversion DisorderDocumento2 páginasConversion DisorderAlya Putri KhairaniAinda não há avaliações
- PSM Bhalani AnswerDocumento423 páginasPSM Bhalani Answerpatilysh1100% (1)
- Dah011 BFD Livestock Diseases (PPP Sept 2021)Documento672 páginasDah011 BFD Livestock Diseases (PPP Sept 2021)Kevin KagambiAinda não há avaliações
- Thyroidinum for Metabolic ImbalancesDocumento4 páginasThyroidinum for Metabolic ImbalancesSuriya OsmanAinda não há avaliações
- Fact File Gastro Intestinal HormonesDocumento2 páginasFact File Gastro Intestinal HormonesSudip DevadasAinda não há avaliações
- Three PointsDocumento5 páginasThree PointscathyAinda não há avaliações
- HyperthyroidismDocumento4 páginasHyperthyroidismavinash dhameriyaAinda não há avaliações
- Nephrotic syndrome: Causes, clinical presentations and histopathologyDocumento53 páginasNephrotic syndrome: Causes, clinical presentations and histopathologyAnna Althafunnisa100% (1)
- Fatigue: Symptom Tiredness Lethargy SleepDocumento10 páginasFatigue: Symptom Tiredness Lethargy Sleepjohnjoseph4069Ainda não há avaliações
- Writing Project 3-5Documento10 páginasWriting Project 3-5api-456365943Ainda não há avaliações
- Personal View: OnlineDocumento9 páginasPersonal View: OnlineMaria YustinaAinda não há avaliações
- Chronic Inflammatory Demyelinating PolyneuropathyDocumento29 páginasChronic Inflammatory Demyelinating PolyneuropathyMarius PapuricaAinda não há avaliações
- Antibiotic Guidelines (2020) - 0Documento55 páginasAntibiotic Guidelines (2020) - 0yudhit bessieAinda não há avaliações
- Case Study Bactegroup 3Documento19 páginasCase Study Bactegroup 3Marjune DimayugaAinda não há avaliações
- 5 Natural Juices To Heal A Sore ThroatDocumento5 páginas5 Natural Juices To Heal A Sore Throatasset68Ainda não há avaliações
- MCB AnswersDocumento10 páginasMCB AnswersLouiegi AlvarezAinda não há avaliações
- Effect of Lactobacillus Gasseri BNR17 On Overweight and Obese Adultts A Randomized, Double-Blind Clinical TrialDocumento10 páginasEffect of Lactobacillus Gasseri BNR17 On Overweight and Obese Adultts A Randomized, Double-Blind Clinical TrialAna Rosa Ortega CastilloAinda não há avaliações
- Biology ProjectDocumento12 páginasBiology Projectvvdgkyezyi100% (1)
- Effectiveness of Behaviour Modification Techniques On Curbing Substance Induced Psychosis at Ngomahuru Psychiatric Hospital.Documento48 páginasEffectiveness of Behaviour Modification Techniques On Curbing Substance Induced Psychosis at Ngomahuru Psychiatric Hospital.tipedzeAinda não há avaliações
- 84359Documento5 páginas84359Pedro Gouveia100% (1)
- Pathology of Diabetic Ketoacidosis - Romeo Rivera Jr.Documento1 páginaPathology of Diabetic Ketoacidosis - Romeo Rivera Jr.romeo riveraAinda não há avaliações
- I. Data Base and History: Bukidnon State UniversityDocumento13 páginasI. Data Base and History: Bukidnon State UniversityJerson BestavillaAinda não há avaliações
- Philippine Medicinal PlantsDocumento62 páginasPhilippine Medicinal PlantsPb100% (2)
- Vocabulary For Med InterpreterDocumento6 páginasVocabulary For Med InterpreterSantiago Ardila-CortesAinda não há avaliações
- Diversity of Avenue PlantingDocumento38 páginasDiversity of Avenue Plantingjoseph Lalremruata100% (1)
- AH2 Hesi ReviewDocumento46 páginasAH2 Hesi ReviewJamie Antonini Grant100% (1)
- Bleeding Disorders: Coagulopathy (Also Called Clotting Disorder and Bleeding DisorderDocumento5 páginasBleeding Disorders: Coagulopathy (Also Called Clotting Disorder and Bleeding DisorderAyisha EdwinAinda não há avaliações
- Soal Bahasa Inggris SNMPTN 2008 101Documento5 páginasSoal Bahasa Inggris SNMPTN 2008 101DittoCendykiaIIAinda não há avaliações
- Bee Stings: The British Beekeepers AssociationDocumento3 páginasBee Stings: The British Beekeepers AssociationantonioforteseAinda não há avaliações