Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- WHO PPHDocumento62 páginasWHO PPHAchyut SharmaAinda não há avaliações
- Dr. Madaan Anatomy MCQ 2-2 (Muhadharaty)Documento46 páginasDr. Madaan Anatomy MCQ 2-2 (Muhadharaty)Joseph Brima SambaAinda não há avaliações
- Professional Plaquex InfoDocumento48 páginasProfessional Plaquex Infoamelia rumenta100% (1)
- Basic Sinus AnatomyDocumento71 páginasBasic Sinus AnatomyTalal AlanzyAinda não há avaliações
- Hematology Oncology - Anemia ApproachDocumento1 páginaHematology Oncology - Anemia ApproachEugen MAinda não há avaliações
- Coagulation Tests: Clotting Time, Bleeding Time, Prothrombin Time, Activated Partial Thromboplastin TimeDocumento15 páginasCoagulation Tests: Clotting Time, Bleeding Time, Prothrombin Time, Activated Partial Thromboplastin TimeAnastasiaAinda não há avaliações
- Textbook of Cardiovascular Medicine in Dogs and Cats (VetBooks - Ir)Documento1.112 páginasTextbook of Cardiovascular Medicine in Dogs and Cats (VetBooks - Ir)Jonathan Mann100% (1)
- The Final FRCR Self-AssessmentDocumento244 páginasThe Final FRCR Self-AssessmentAman KumarAinda não há avaliações
- Mycoplasmic Theory of Rheumatoid DiseaseDocumento81 páginasMycoplasmic Theory of Rheumatoid DiseaseChristopher Phillips100% (1)
- Emergency TrollyDocumento26 páginasEmergency Trollyahmshm50% (4)
- Rinitis 2011. ARIA.Documento6 páginasRinitis 2011. ARIA.Hans CruzAinda não há avaliações
- Diagnóstico Radiológico de Apendicitis Aguda: RadiologiaDocumento3 páginasDiagnóstico Radiológico de Apendicitis Aguda: RadiologiaAnonymous envUOdVAinda não há avaliações
- Shock HemorragicoDocumento29 páginasShock HemorragicoHans CruzAinda não há avaliações
- Anemia en Enfermedad Cardiaca AHADocumento10 páginasAnemia en Enfermedad Cardiaca AHAHans CruzAinda não há avaliações
- Poliradiculopatia Inflamatoria DesmielinizanteDocumento6 páginasPoliradiculopatia Inflamatoria DesmielinizanteHans CruzAinda não há avaliações
- KDIGO Lipid Management Guideline 2013Documento56 páginasKDIGO Lipid Management Guideline 2013Manuel MoralesAinda não há avaliações
- KDIGO Lipid Management Guideline 2013Documento56 páginasKDIGO Lipid Management Guideline 2013Manuel MoralesAinda não há avaliações
- Guia de Tratamiento AHA/ACC para Pacientes Con Sidrome Coronario Sin Elevacion Del STDocumento83 páginasGuia de Tratamiento AHA/ACC para Pacientes Con Sidrome Coronario Sin Elevacion Del STHans CruzAinda não há avaliações
- Uso de Opioides en Tratamiento de Dolor CronicoDocumento9 páginasUso de Opioides en Tratamiento de Dolor CronicoHans CruzAinda não há avaliações
- Lab 2 - Birth Spacing Policy in OmanDocumento39 páginasLab 2 - Birth Spacing Policy in OmanMeme 1234Ainda não há avaliações
- Digestive System AnatomyDocumento30 páginasDigestive System AnatomyPranali BasuAinda não há avaliações
- Nursing Care Plan Drug Study: Assessment Nursing Diagnosis Nursing Goal Nursing Intervention Rationale EvaluationDocumento2 páginasNursing Care Plan Drug Study: Assessment Nursing Diagnosis Nursing Goal Nursing Intervention Rationale Evaluationteejay andradaAinda não há avaliações
- SGD Gross AnatomyDocumento11 páginasSGD Gross Anatomyluis_chubeeAinda não há avaliações
- Pipeline_Update_30JAN2024_0Documento19 páginasPipeline_Update_30JAN2024_0RC CharlesAinda não há avaliações
- Nur 111 Session 7 Sas 1Documento8 páginasNur 111 Session 7 Sas 1Zzimply Tri Sha UmaliAinda não há avaliações
- Nyeri Dada Dalam Klinis Sehari HariDocumento35 páginasNyeri Dada Dalam Klinis Sehari Hariknzt613Ainda não há avaliações
- Fifteen Years Experience With Finger Arterial Pressure MonitoringDocumento12 páginasFifteen Years Experience With Finger Arterial Pressure MonitoringLevente BalázsAinda não há avaliações
- Twin To Twin Transfusion PDFDocumento26 páginasTwin To Twin Transfusion PDFAmbreen Z MalikAinda não há avaliações
- Vol 1 No 1Documento432 páginasVol 1 No 1cslee100% (1)
- GRAND TotalDocumento35 páginasGRAND TotalNoveeAinda não há avaliações
- Final Coaching CardioDocumento70 páginasFinal Coaching CardiomarykristiroseAinda não há avaliações
- Module 4 - Approach To The Comatose PatientDocumento35 páginasModule 4 - Approach To The Comatose PatientRick RanitAinda não há avaliações
- Surgery-I Review (2019)Documento12 páginasSurgery-I Review (2019)Margaret ThatcherAinda não há avaliações
- Biology Worksheet Sheep Heart DissectionDocumento3 páginasBiology Worksheet Sheep Heart DissectionFluphie Bunny0% (1)
- LIVERDocumento106 páginasLIVERCurt Leye RodriguezAinda não há avaliações
- Haematological Parameters and Lipid Profile AbnormDocumento10 páginasHaematological Parameters and Lipid Profile AbnormPhelix O DaniyanAinda não há avaliações
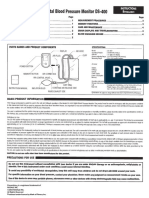
- Digital Blood Pressure Monitor DS-400: Parts Names and Product ComponentsDocumento4 páginasDigital Blood Pressure Monitor DS-400: Parts Names and Product ComponentsJorAinda não há avaliações
- Cardiovascular Research Convergence 2022Documento16 páginasCardiovascular Research Convergence 2022Aditya SutarAinda não há avaliações
- LEONCITO - Module 16 Worksheets 2Documento12 páginasLEONCITO - Module 16 Worksheets 2Anton LeoncitoAinda não há avaliações
- Medical Terminogy: Assignment - 1Documento5 páginasMedical Terminogy: Assignment - 1Vineet SinghAinda não há avaliações