Você também pode gostar
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Calculating Forklift Aisle Width MinimumsDocumento2 páginasCalculating Forklift Aisle Width Minimumsraju1559405Ainda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- PROSOLV-tech Info Prosolv Func Inv GB 1809Documento12 páginasPROSOLV-tech Info Prosolv Func Inv GB 1809raju1559405Ainda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- GEA-Article - Courtoy MUPS - Innovation in Pharmaceutical TechnologyDocumento3 páginasGEA-Article - Courtoy MUPS - Innovation in Pharmaceutical Technologyraju1559405Ainda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Order Picking: Safe Work GuidelinesDocumento5 páginasOrder Picking: Safe Work Guidelinesraju1559405Ainda não há avaliações
- Reactivity QuinolineDocumento107 páginasReactivity QuinolineIan Otto100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Manufacturing Process Scale UpDocumento5 páginasManufacturing Process Scale Upraju1559405Ainda não há avaliações
- Manufacturing Process Scale UpDocumento5 páginasManufacturing Process Scale Upraju1559405Ainda não há avaliações
- The Work of Eurovent: What's in Eurovent?Documento3 páginasThe Work of Eurovent: What's in Eurovent?raju1559405Ainda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Training-Coating Machine OperationDocumento12 páginasTraining-Coating Machine Operationraju1559405Ainda não há avaliações
- Operational Performance and Optimization of RO Wastewater Treatment PlantsDocumento12 páginasOperational Performance and Optimization of RO Wastewater Treatment PlantsalesclAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- GEA-The Reality of Continuous Pharmaceutical Manufacturing Conference - Hosted by GEA, Siemens & Perceptive EngineeringDocumento4 páginasGEA-The Reality of Continuous Pharmaceutical Manufacturing Conference - Hosted by GEA, Siemens & Perceptive Engineeringraju1559405Ainda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- GEA-Article - Courtoy MUPS - Innovation in Pharmaceutical TechnologyDocumento3 páginasGEA-Article - Courtoy MUPS - Innovation in Pharmaceutical Technologyraju1559405Ainda não há avaliações
- Mobile Pharmaceutical Work StationDocumento4 páginasMobile Pharmaceutical Work Stationraju1559405Ainda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- HeatingDocumento134 páginasHeatingraju1559405Ainda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- FiveDocumento8 páginasFiveraju1559405Ainda não há avaliações
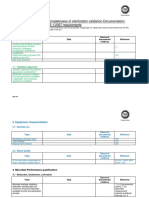
- Demand of Pharmaceutical Facility Functionality - Validation and Qualification of HVAC SystemDocumento17 páginasDemand of Pharmaceutical Facility Functionality - Validation and Qualification of HVAC Systemraju1559405Ainda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- SurgicalDocumento3 páginasSurgicalraju1559405Ainda não há avaliações
- AIA Guidelines Patient Care Construction Air ChangeDocumento2 páginasAIA Guidelines Patient Care Construction Air ChangeMinh van LeAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- 349 893 1 SMDocumento5 páginas349 893 1 SMrambabuAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Fgi Guidelines 2014 Hop TocDocumento10 páginasFgi Guidelines 2014 Hop TocZaw Moe KhineAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Aia Guidelines Patient VentilationDocumento3 páginasAia Guidelines Patient Ventilationraju1559405Ainda não há avaliações
- Eurovent-Rating Standard For The Certification of Air Handling Units - rs-6c005-2016 - AhuDocumento3 páginasEurovent-Rating Standard For The Certification of Air Handling Units - rs-6c005-2016 - Ahuraju1559405Ainda não há avaliações
- Autocad ShortcutsDocumento13 páginasAutocad ShortcutsKriscel CaraanAinda não há avaliações
- Demand of Pharmaceutical Facility Functionality - Validation and Qualification of HVAC SystemDocumento17 páginasDemand of Pharmaceutical Facility Functionality - Validation and Qualification of HVAC Systemraju1559405Ainda não há avaliações
- 349 893 1 SMDocumento5 páginas349 893 1 SMrambabuAinda não há avaliações
- EUROVENT Programme DescriptionsDocumento1 páginaEUROVENT Programme Descriptionsraju1559405Ainda não há avaliações
- How Efficient Is Your Boiler HouseDocumento3 páginasHow Efficient Is Your Boiler Houseraju1559405Ainda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (120)
- Ultra Pure Water Treatment For Pharmaceutical IndustryDocumento4 páginasUltra Pure Water Treatment For Pharmaceutical Industryraju1559405100% (1)
- Microbiological Assessment of Compressed Gases in Pharmaceutical FacilitiesDocumento6 páginasMicrobiological Assessment of Compressed Gases in Pharmaceutical Facilitiesraju1559405Ainda não há avaliações
- Sampling Water Table ContentsDocumento2 páginasSampling Water Table Contentsraju1559405Ainda não há avaliações
- Bio-Burden Test Procedure.: Revital Healthcare (Epz) LTDDocumento5 páginasBio-Burden Test Procedure.: Revital Healthcare (Epz) LTDMusyoka UrbanusAinda não há avaliações
- 05 Gamma Dose Auditing For 11137 2006 Method 1Documento3 páginas05 Gamma Dose Auditing For 11137 2006 Method 1601026Ainda não há avaliações
- Assuring Sterility With ASTM F 838-83Documento6 páginasAssuring Sterility With ASTM F 838-83Iin Tirta SunartaAinda não há avaliações
- Sops IndexDocumento3 páginasSops IndexIbrahim IssaAinda não há avaliações
- 7.overview of Filter Validation-K.michaelDocumento62 páginas7.overview of Filter Validation-K.michaelqhpuongAinda não há avaliações
- Gamma Radiation SterilizationDocumento2 páginasGamma Radiation Sterilizationananth67% (3)
- Bioburden TestDocumento4 páginasBioburden TestMujeeb Ullah KhanAinda não há avaliações
- 6 Microbial Requirements and Testing of Primary Packaging: Marcel GoverdeDocumento36 páginas6 Microbial Requirements and Testing of Primary Packaging: Marcel GoverdeQA QCAinda não há avaliações
- West Flip Off Seal Challenger Sell SheetDocumento2 páginasWest Flip Off Seal Challenger Sell SheetKamalAinda não há avaliações
- Sterilization Review Questionnaire ETODocumento5 páginasSterilization Review Questionnaire ETOsaberAinda não há avaliações
- Identifying Sterilizing FilterDocumento7 páginasIdentifying Sterilizing FilterMWJornitz100% (1)
- IDFL Test Summary - Bioburden A4Documento1 páginaIDFL Test Summary - Bioburden A4Keith WilsonAinda não há avaliações
- Bio Burden TestingDocumento1 páginaBio Burden TestingRoxanaBurlaAinda não há avaliações
- Microbiological Test of Medical DevicesDocumento5 páginasMicrobiological Test of Medical Devicesbijendra_sinhaAinda não há avaliações
- 394 in Process Revision 1115 Bioburden Control of Nonsterile Drug Substances and ProductsDocumento9 páginas394 in Process Revision 1115 Bioburden Control of Nonsterile Drug Substances and Productsdeepanmb007Ainda não há avaliações
- Validation of Sterile Filtration ArticleDocumento10 páginasValidation of Sterile Filtration Articleortizan8Ainda não há avaliações
- 1222 Terminal SterilizationDocumento4 páginas1222 Terminal SterilizationSpectre SpectreAinda não há avaliações
- Sterilization Overkill ApproachDocumento11 páginasSterilization Overkill ApproachVijay100% (2)
- Usp42-Nf37 218Documento3 páginasUsp42-Nf37 218Mohamed HassanAinda não há avaliações
- Presenatation - MICROBIOLOGICAL TESTING IN PHARMACEUTICAL INDUSTRIESDocumento20 páginasPresenatation - MICROBIOLOGICAL TESTING IN PHARMACEUTICAL INDUSTRIESqurat0405Ainda não há avaliações
- ECA Task Force CCS GuidelineDocumento48 páginasECA Task Force CCS Guidelinemercedes100% (1)
- The Role of Microbiology in The Design and Development of Pharmaceutical Manufacturing ProcessesDocumento4 páginasThe Role of Microbiology in The Design and Development of Pharmaceutical Manufacturing ProcessesHari RamAinda não há avaliações
- Valid Sterisart-NF SLD5704-eDocumento67 páginasValid Sterisart-NF SLD5704-esizhusyAinda não há avaliações
- SOP For Bioburden TestDocumento2 páginasSOP For Bioburden TestBejoy KarimAinda não há avaliações
- Readytoprocess NFFDocumento8 páginasReadytoprocess NFFAnil ReddyAinda não há avaliações
- Environmental Monitoring and Microbiological Manufacture of Sterile DrugsDocumento8 páginasEnvironmental Monitoring and Microbiological Manufacture of Sterile DrugsKristian Uriel DelgadoAinda não há avaliações
- Radiation Dose Setting - Tech TipDocumento6 páginasRadiation Dose Setting - Tech Tipjchav004ucrAinda não há avaliações
- Cases Study of Microbiological Contamination2011Documento8 páginasCases Study of Microbiological Contamination2011Cristina Croitoru0% (1)
- The Voice of God: Experience A Life Changing Relationship with the LordNo EverandThe Voice of God: Experience A Life Changing Relationship with the LordAinda não há avaliações
- Confinement (Book #1 in the Love and Madness series)No EverandConfinement (Book #1 in the Love and Madness series)Ainda não há avaliações