Você também pode gostar
- 08 Common Problems That Develop During InfancyDocumento48 páginas08 Common Problems That Develop During InfancyLorelie AsisAinda não há avaliações
- No Gallbladder Diet Cookbook: Discover Flavorful and Nourishing Recipes to Revitalize Your Metabolism After Gallbladder Surgery [III EDITION]No EverandNo Gallbladder Diet Cookbook: Discover Flavorful and Nourishing Recipes to Revitalize Your Metabolism After Gallbladder Surgery [III EDITION]Nota: 5 de 5 estrelas5/5 (24)
- Abdominal Wall DefectsDocumento20 páginasAbdominal Wall DefectsxylomiteAinda não há avaliações
- Common Pediatric Surgery ProblemsDocumento141 páginasCommon Pediatric Surgery Problemssedaka26100% (4)
- Congenital Anomalies of GiDocumento94 páginasCongenital Anomalies of GiPadmaAinda não há avaliações
- Strangulation Assessment Evidence Collection and Documentation PDFDocumento36 páginasStrangulation Assessment Evidence Collection and Documentation PDFBoţu AlexandruAinda não há avaliações
- Surgery - Pediatric GIT, Abdominal Wall, Neoplasms - 2014ADocumento14 páginasSurgery - Pediatric GIT, Abdominal Wall, Neoplasms - 2014ATwinkle SalongaAinda não há avaliações
- Ligature Strangulation - StudentsDocumento28 páginasLigature Strangulation - StudentsBoţu Alexandru100% (1)
- Approach To Abdominal Masses in ChildrenDocumento36 páginasApproach To Abdominal Masses in ChildrenMia Lesaca-Medina100% (3)
- Congenital AnomaliesDocumento39 páginasCongenital Anomaliesiqiqiqiqiq100% (1)
- Abdominal Wall DefectsDocumento16 páginasAbdominal Wall DefectsDesta FransiscaAinda não há avaliações
- Duodenal AtresiaDocumento18 páginasDuodenal AtresiaRianto Noviady RamliAinda não há avaliações
- Prune Belly SyndromeDocumento39 páginasPrune Belly SyndromeHudaAinda não há avaliações
- IntussusceptionDocumento19 páginasIntussusceptionarialAinda não há avaliações
- GI Clinical Case ConferenceDocumento42 páginasGI Clinical Case ConferencemasmblinkAinda não há avaliações
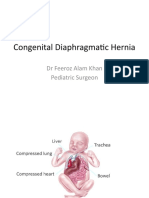
- Congenital Diaphragmatic Hernia: DR Feeroz Alam Khan Pediatric SurgeonDocumento21 páginasCongenital Diaphragmatic Hernia: DR Feeroz Alam Khan Pediatric SurgeonPrabhat GuptaAinda não há avaliações
- Gastro NephroDocumento93 páginasGastro Nephrohasanatiya41Ainda não há avaliações
- Omphalocelevsgastroschisis 160810122732Documento23 páginasOmphalocelevsgastroschisis 160810122732LNICCOLAIO100% (1)
- Neonatal Intestinal Obstruction EPSGHAN PDFDocumento77 páginasNeonatal Intestinal Obstruction EPSGHAN PDFRobert ChristevenAinda não há avaliações
- 19-Pediatric SurgeryDocumento39 páginas19-Pediatric Surgerycallisto3487Ainda não há avaliações
- Gastroschizis Vs OmfalocelDocumento35 páginasGastroschizis Vs OmfalocelElena LicsandruAinda não há avaliações
- 20 PediatricDocumento31 páginas20 PediatricMahmoud AbuAwadAinda não há avaliações
- Duodenal Obstruction: Dr. Mochamad Reza FebrianDocumento24 páginasDuodenal Obstruction: Dr. Mochamad Reza FebrianBoby ChandraAinda não há avaliações
- Preoperative & Postoperative EvaluationDocumento61 páginasPreoperative & Postoperative EvaluationSonntagsschule St. Antonius Kloster in KröffelbachAinda não há avaliações
- Pediatric SurgeryDocumento60 páginasPediatric SurgeryAbdalla SamatarAinda não há avaliações
- Neonatal Anaesthesia 2 Anaesthesia For Neonates With Abdominal Wall DefectsDocumento10 páginasNeonatal Anaesthesia 2 Anaesthesia For Neonates With Abdominal Wall DefectsDr. Anish GolchhaAinda não há avaliações
- Problem 4 Git: Ivan Michael (405090161)Documento22 páginasProblem 4 Git: Ivan Michael (405090161)vnAinda não há avaliações
- Abdominal Wall Defects: Omphalocele GastroschisisDocumento20 páginasAbdominal Wall Defects: Omphalocele GastroschisisYogi drAinda não há avaliações
- Common Congenital Git Malformations FinDocumento60 páginasCommon Congenital Git Malformations FinRuth DanielAinda não há avaliações
- Abdominal Wall Defects: Dr. Catherine B. CaneteDocumento42 páginasAbdominal Wall Defects: Dr. Catherine B. CaneteLuqman AlwiAinda não há avaliações
- Abdominal Wall Defects PresentationDocumento45 páginasAbdominal Wall Defects PresentationWasswaAinda não há avaliações
- Hirschsprung DiseaseDocumento20 páginasHirschsprung DiseaseIvy DanAinda não há avaliações
- Pemeriksaan Rontgen Toraks, Elektrokardiogram (EKG), USG Abdomen Dan EchocardiografiDocumento5 páginasPemeriksaan Rontgen Toraks, Elektrokardiogram (EKG), USG Abdomen Dan EchocardiografigorodoeAinda não há avaliações
- Comparison of Transverse and Vertical Skin Incision ForDocumento6 páginasComparison of Transverse and Vertical Skin Incision ForHerry SasukeAinda não há avaliações
- Abnormalities in Small Bowel: Dr. Iqbal Pahlevi, SPB, SpbaDocumento36 páginasAbnormalities in Small Bowel: Dr. Iqbal Pahlevi, SPB, SpbafinikollinsAinda não há avaliações
- Genitourinary Alterations in Chldren: Heather BuccelloDocumento46 páginasGenitourinary Alterations in Chldren: Heather BuccelloshanikaAinda não há avaliações
- Mwima Ongaro VincentDocumento17 páginasMwima Ongaro VincentMalueth AnguiAinda não há avaliações
- Abdominal Wall DEFECTS: Omphalocele, Gastroschisis, Prune-BellyDocumento38 páginasAbdominal Wall DEFECTS: Omphalocele, Gastroschisis, Prune-BellyWorku KifleAinda não há avaliações
- Large Bowel Obstruction: Katherine Jahnes MD Colorectal Conference ST Luke's Roosevelt Hospital Center November 10, 2005Documento22 páginasLarge Bowel Obstruction: Katherine Jahnes MD Colorectal Conference ST Luke's Roosevelt Hospital Center November 10, 2005samsabesAinda não há avaliações
- GERD in ChildrenDocumento31 páginasGERD in ChildrenSalman KhanAinda não há avaliações
- Emergencies in GITDocumento7 páginasEmergencies in GITsssajiAinda não há avaliações
- Asfiksia PerinatalDocumento63 páginasAsfiksia PerinatalrantiadrianiAinda não há avaliações
- Hirschprung DiseaseDocumento9 páginasHirschprung DiseaseJonathan ObañaAinda não há avaliações
- Anaesthetic Management of Paediatric Emergencies Corrected 3Documento51 páginasAnaesthetic Management of Paediatric Emergencies Corrected 3oriaboseAinda não há avaliações
- TRUMADocumento56 páginasTRUMAzainabd1964Ainda não há avaliações
- Abdominal Wall Defects 5 17Documento26 páginasAbdominal Wall Defects 5 17Roqoyyah MursyidAinda não há avaliações
- Acute Appendicitis: Resident: DR SD Sanyal Moderator: Brig SR Ghosh Consultant Surgery and GI SurgeonDocumento50 páginasAcute Appendicitis: Resident: DR SD Sanyal Moderator: Brig SR Ghosh Consultant Surgery and GI SurgeonAku IyunkAinda não há avaliações
- Meckel's Diverticulum DR SuryaDocumento30 páginasMeckel's Diverticulum DR SuryaHorakhty PrideAinda não há avaliações
- Congenital Diaphragmatic HerniaDocumento45 páginasCongenital Diaphragmatic HerniaDabessa MosissaAinda não há avaliações
- Vomiting in InfantDocumento44 páginasVomiting in InfantsilviafarraposoAinda não há avaliações
- Abdominal PainDocumento6 páginasAbdominal PainMatthieu FortinAinda não há avaliações
- Test 2 NotesDocumento38 páginasTest 2 Notesbjpalmer100% (2)
- Acute Appendicectomy: Click To Edit Master Subtitle StyleDocumento38 páginasAcute Appendicectomy: Click To Edit Master Subtitle StyleSiti Khadijah MustaphaAinda não há avaliações
- PEDI 2. Embryologic Basis of GI Malformations 2021Documento54 páginasPEDI 2. Embryologic Basis of GI Malformations 2021Hayle MaryamAinda não há avaliações
- Kelainan Kongenital GI & HepatobilierDocumento43 páginasKelainan Kongenital GI & HepatobilierhusnaaAinda não há avaliações
- BR Feto I IYADocumento21 páginasBR Feto I IYAshare fosAinda não há avaliações
- Abdominal Wall DefectsDocumento27 páginasAbdominal Wall Defectstsega tilahunAinda não há avaliações
- Ohss 2014Documento67 páginasOhss 2014Dima AtabehAinda não há avaliações
- Journal Reading BEdah AnakDocumento19 páginasJournal Reading BEdah AnaktomyeffendiAinda não há avaliações
- Gastroenterology For General SurgeonsNo EverandGastroenterology For General SurgeonsMatthias W. WichmannAinda não há avaliações
- PrefaceDocumento2 páginasPrefaceBoţu AlexandruAinda não há avaliações
- CH 7Documento30 páginasCH 7Boţu AlexandruAinda não há avaliações
- CH 13Documento22 páginasCH 13Boţu AlexandruAinda não há avaliações
- CH 9Documento18 páginasCH 9Boţu AlexandruAinda não há avaliações
- CH 4Documento22 páginasCH 4Boţu AlexandruAinda não há avaliações
- CH 5Documento18 páginasCH 5Boţu AlexandruAinda não há avaliações
- CH 6Documento16 páginasCH 6Boţu AlexandruAinda não há avaliações
- Jalt13i1p63 PDFDocumento3 páginasJalt13i1p63 PDFBoţu AlexandruAinda não há avaliações
- Curs 4 Urgente in Cardiologie Anul VI Seriile A B C DDocumento35 páginasCurs 4 Urgente in Cardiologie Anul VI Seriile A B C DBoţu AlexandruAinda não há avaliações
- A Rareposition in Partial Hanging - A Case ReportDocumento4 páginasA Rareposition in Partial Hanging - A Case ReportBoţu AlexandruAinda não há avaliações
- Introduction To Forensic Science Lecture 5 Forensic PathologyDocumento89 páginasIntroduction To Forensic Science Lecture 5 Forensic PathologyBoţu Alexandru100% (4)
- Forensic Medical Findings in Fatal and Non-Fatal Intimate Partner Strangulation Assaults - Hawley - 2012 PDFDocumento20 páginasForensic Medical Findings in Fatal and Non-Fatal Intimate Partner Strangulation Assaults - Hawley - 2012 PDFBoţu AlexandruAinda não há avaliações

![No Gallbladder Diet Cookbook: Discover Flavorful and Nourishing Recipes to Revitalize Your Metabolism After Gallbladder Surgery [III EDITION]](https://imgv2-2-f.scribdassets.com/img/word_document/591540228/149x198/6ba6cc3b38/1713999276?v=1)