Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- 68-year-old Man with Breathing Problems Due to IV Fluid OverdoseDocumento3 páginas68-year-old Man with Breathing Problems Due to IV Fluid OverdoseAnna-Marie Hanson100% (15)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- 002367889dissecting The USMLE - BookmarkedDocumento629 páginas002367889dissecting The USMLE - BookmarkedPharAway100% (6)
- Adrenal Function TestDocumento26 páginasAdrenal Function TestSaroja Veeresh83% (6)
- Problems of Choice IJSDL 3.2Documento63 páginasProblems of Choice IJSDL 3.2Edvard LjulkoAinda não há avaliações
- 34319Documento11 páginas34319Akbar GazaliAinda não há avaliações
- Self-Directed Learning Scale For Nurses-AanDocumento10 páginasSelf-Directed Learning Scale For Nurses-AanAkbar GazaliAinda não há avaliações
- Rice Spearman DissertationDocumento102 páginasRice Spearman DissertationAkbar Gazali100% (1)
- July 1991 GDocumento5 páginasJuly 1991 GAkbar GazaliAinda não há avaliações
- Neonatal Respiratory Distress 4Documento4 páginasNeonatal Respiratory Distress 4Akbar GazaliAinda não há avaliações
- Educational Strategies Associated With Development of Problem-Solving, Critical Thinking, and Self-Directed LearningDocumento12 páginasEducational Strategies Associated With Development of Problem-Solving, Critical Thinking, and Self-Directed LearningAkbar GazaliAinda não há avaliações
- Full TextDocumento116 páginasFull TextAkbar GazaliAinda não há avaliações
- Epistemological Beliefs and Self-Directed LearningDocumento138 páginasEpistemological Beliefs and Self-Directed LearningAkbar GazaliAinda não há avaliações
- Review Article: Tuberculous Meningitis: Diagnosis and Treatment OverviewDocumento10 páginasReview Article: Tuberculous Meningitis: Diagnosis and Treatment OverviewMeldaAinda não há avaliações
- Antibiotic For AURIDocumento11 páginasAntibiotic For AURIYani Dwi PratiwiAinda não há avaliações
- Growth Chart For Boys Birth To 36 MonthsDocumento2 páginasGrowth Chart For Boys Birth To 36 MonthsCarlos TejedaAinda não há avaliações
- Full TextDocumento116 páginasFull TextAkbar GazaliAinda não há avaliações
- CG 69 Full GuidelineDocumento121 páginasCG 69 Full GuidelineIras Diah DiahAinda não há avaliações
- Acute Flaccid ParalysisDocumento3 páginasAcute Flaccid ParalysisMobin Ur Rehman KhanAinda não há avaliações
- Review Article: Tuberculous Meningitis: Diagnosis and Treatment OverviewDocumento10 páginasReview Article: Tuberculous Meningitis: Diagnosis and Treatment OverviewMeldaAinda não há avaliações
- 01-04-14 KetDocumento6 páginas01-04-14 KetAkbar GazaliAinda não há avaliações
- Revisi MR Akbar 12 Mei 2014 Kala I Fase Aktif Macet + Retensio Plasenta Dan IUGRDocumento31 páginasRevisi MR Akbar 12 Mei 2014 Kala I Fase Aktif Macet + Retensio Plasenta Dan IUGRAkbar GazaliAinda não há avaliações
- Name: Mrs. E Age: 26 Yo RM: 538866 Adress: Narmada Admitted: May, 18 2012 at 02.51 Name: Mrs. E Age: 26 Yo RM: 538866 Adress: Narmada Admitted: May, 18 2012 at 02.51Documento5 páginasName: Mrs. E Age: 26 Yo RM: 538866 Adress: Narmada Admitted: May, 18 2012 at 02.51 Name: Mrs. E Age: 26 Yo RM: 538866 Adress: Narmada Admitted: May, 18 2012 at 02.51Akbar GazaliAinda não há avaliações
- Morning Report March, 24: Supervisor: Dr.H. Doddy A.K., Spog DM: Akbar, Ariq, AsriDocumento9 páginasMorning Report March, 24: Supervisor: Dr.H. Doddy A.K., Spog DM: Akbar, Ariq, AsriAkbar GazaliAinda não há avaliações
- Vol11No2 Pg68-69Documento2 páginasVol11No2 Pg68-69ikawyuAinda não há avaliações
- Supervisor: Dr. Agus Thoriq, Spog DM: AkbarDocumento31 páginasSupervisor: Dr. Agus Thoriq, Spog DM: AkbarAkbar GazaliAinda não há avaliações
- 21-03-14 KPD + Atonia UteriDocumento18 páginas21-03-14 KPD + Atonia UteriAkbar GazaliAinda não há avaliações
- 22-02-14 KPD + OligohidramnionDocumento12 páginas22-02-14 KPD + OligohidramnionAkbar GazaliAinda não há avaliações
- Supervisor: Dr. Juliawan, Spog DM: Ery, Heri, Mamat, AsriDocumento11 páginasSupervisor: Dr. Juliawan, Spog DM: Ery, Heri, Mamat, AsriAkbar GazaliAinda não há avaliações
- 28-02-14 PK I F.latenDocumento12 páginas28-02-14 PK I F.latenAkbar GazaliAinda não há avaliações
- 21-03-14 KPD + Atonia UteriDocumento18 páginas21-03-14 KPD + Atonia UteriAkbar GazaliAinda não há avaliações
- MR Jaga Sabtu 17 Mei 2014Documento10 páginasMR Jaga Sabtu 17 Mei 2014Akbar GazaliAinda não há avaliações
- Morning Report March, 24: Supervisor: Dr.H. Doddy A.K., Spog DM: Akbar, Ariq, AsriDocumento9 páginasMorning Report March, 24: Supervisor: Dr.H. Doddy A.K., Spog DM: Akbar, Ariq, AsriAkbar GazaliAinda não há avaliações
- Negative Feedback - Wikipedia, The Free Encyclopedia PDFDocumento11 páginasNegative Feedback - Wikipedia, The Free Encyclopedia PDFVanessa HollandAinda não há avaliações
- Endocrine SystemDocumento24 páginasEndocrine Systemapi-290318217Ainda não há avaliações
- 45 Lecture PresentationDocumento95 páginas45 Lecture PresentationCourtney TaylorAinda não há avaliações
- Endocrine System - outlINEDocumento4 páginasEndocrine System - outlINERalph NilloAinda não há avaliações
- Endocrinology InterpretationDocumento382 páginasEndocrinology InterpretationHernanda Adi Purwangga100% (7)
- Assessing Clients with Endocrine and Metabolic DisordersDocumento4 páginasAssessing Clients with Endocrine and Metabolic DisordersFelimon BugtongAinda não há avaliações
- New Advances in Diagnosis and Treatment of Cushing SyndromeDocumento12 páginasNew Advances in Diagnosis and Treatment of Cushing SyndromeIka AnisaAinda não há avaliações
- Endocrine SystemDocumento11 páginasEndocrine SystemPunong Grande NHS Banga NHS Annex (R XII - South Cotabato)Ainda não há avaliações
- What Is Adrenal InsufficiencyDocumento17 páginasWhat Is Adrenal InsufficiencygammuacAinda não há avaliações
- Cushing's DiseaseDocumento1 páginaCushing's DiseaseAdeline N. OmeneAinda não há avaliações
- Benefits and Harm of Systemic Steroids For ShortDocumento27 páginasBenefits and Harm of Systemic Steroids For ShortSebastian DíazAinda não há avaliações
- CH 52 Assessment and Management of Patients With Endocrine DisordersDocumento15 páginasCH 52 Assessment and Management of Patients With Endocrine Disordersfiya33Ainda não há avaliações
- Endocrine Dysfunction: Adrenal & Pituitary: Endocrine System Endocrine ReviewDocumento102 páginasEndocrine Dysfunction: Adrenal & Pituitary: Endocrine System Endocrine ReviewCalimlim KimAinda não há avaliações
- 2011 Semifinal AnswersDocumento43 páginas2011 Semifinal AnswersSamsamaAinda não há avaliações
- Adrenal Gland DisordersDocumento3 páginasAdrenal Gland DisordersJem Fabico Dee-AhrAinda não há avaliações
- Overtraining Syndrome in The Athlete: Current Clinical PracticeDocumento7 páginasOvertraining Syndrome in The Athlete: Current Clinical PracticeJosé Luis OjedaAinda não há avaliações
- Consideration of Steroids For Endodontic Pain MarshallDocumento11 páginasConsideration of Steroids For Endodontic Pain MarshallcarlafacchinAinda não há avaliações
- Impact of Stress Management on Student LearningDocumento33 páginasImpact of Stress Management on Student LearningImran100% (1)
- The Mechanisms of Postpartum DepressionDocumento70 páginasThe Mechanisms of Postpartum Depressionazniahsyam8269Ainda não há avaliações
- Clinical BiochemistryDocumento71 páginasClinical BiochemistryMuhamed ArsalanAinda não há avaliações
- Alterations in Physiology and Anatomy During Pregnancy PDFDocumento12 páginasAlterations in Physiology and Anatomy During Pregnancy PDFAsh AmeAinda não há avaliações
- PPT All Endocrine PharmacologyDocumento143 páginasPPT All Endocrine PharmacologyabenezergebrekirstosAinda não há avaliações
- The Slings and Arrows of Daily LifeDocumento17 páginasThe Slings and Arrows of Daily Lifeneurogenics_18570782Ainda não há avaliações
- American Handbook of Psychiatry - Vol7 PDFDocumento2.079 páginasAmerican Handbook of Psychiatry - Vol7 PDFLidia Maria BăloiAinda não há avaliações
- Chapter11 PDFDocumento24 páginasChapter11 PDFsgw67Ainda não há avaliações
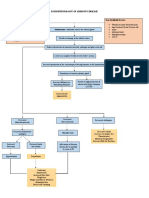
- Pathophysiology of Addison's Disease ExplainedDocumento2 páginasPathophysiology of Addison's Disease ExplainedHanna NocumAinda não há avaliações
- Endocrine SystemDocumento3 páginasEndocrine Systemyessii_rahmawatiAinda não há avaliações