Você também pode gostar
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- Body TissuesDocumento29 páginasBody TissuesPurplesmilezAinda não há avaliações
- CBSE Quick Revision Notes (Class-11 Biology) Chapter-22 Chemical Coordination and IntegrationDocumento3 páginasCBSE Quick Revision Notes (Class-11 Biology) Chapter-22 Chemical Coordination and IntegrationNANDAKUMAR BABUAinda não há avaliações
- Health Education - CholelithiasisDocumento12 páginasHealth Education - Cholelithiasismohamad dildarAinda não há avaliações
- Principles of Anatomy and Physiology: 14 EditionDocumento62 páginasPrinciples of Anatomy and Physiology: 14 EditionWilliam C Chisha100% (1)
- Rest and SleepDocumento11 páginasRest and Sleepdlneisha61Ainda não há avaliações
- Sterilization and DisinfectionDocumento24 páginasSterilization and DisinfectionMrs RehanAinda não há avaliações
- Circulatory System FrogDocumento9 páginasCirculatory System FrogLeticiaAinda não há avaliações
- Sponge BathDocumento16 páginasSponge Bathnamrata kAinda não há avaliações
- Endocrine SystemDocumento6 páginasEndocrine SystemChechan AmbaAinda não há avaliações
- Clear Liquid Diet: PurposeDocumento10 páginasClear Liquid Diet: PurposeJoyVee Pillagara-De LeonAinda não há avaliações
- Anatomy of The Reproductive System EDocumento4 páginasAnatomy of The Reproductive System EshreeAinda não há avaliações
- The-Skull by Dr. Phan SandethDocumento65 páginasThe-Skull by Dr. Phan SandethTith Sunny100% (2)
- Procedure Checklist On Tracheostomy CareDocumento2 páginasProcedure Checklist On Tracheostomy CareDoc Zay VillafuerteAinda não há avaliações
- An Organ That Receives and Relays Information About The Body's Senses To The BrainDocumento59 páginasAn Organ That Receives and Relays Information About The Body's Senses To The BrainIsarra AmsaluAinda não há avaliações
- Open Bed MakingDocumento3 páginasOpen Bed MakingAparna HarshanAinda não há avaliações
- CholeraDocumento4 páginasCholeraBeth AvelinoAinda não há avaliações
- Specimen Collection Print PDFDocumento8 páginasSpecimen Collection Print PDFgeehan Ahmed100% (1)
- Musculo Care Modalities 2 PDFDocumento44 páginasMusculo Care Modalities 2 PDFAhmad FaujiAinda não há avaliações
- Otitis MediaDocumento9 páginasOtitis MediaMona Santi NainggolanAinda não há avaliações
- Lymphatic SystemDocumento5 páginasLymphatic SystemCurex QAAinda não há avaliações
- Health AssessmentDocumento2 páginasHealth AssessmentrojeanrubinoAinda não há avaliações
- Physiology of ThyroidDocumento9 páginasPhysiology of ThyroidAbby EvangelistaAinda não há avaliações
- 2 Infection ControlDocumento34 páginas2 Infection ControlMustapha S. MintehAinda não há avaliações
- Neurological Assessment PDFDocumento52 páginasNeurological Assessment PDFJosephine George JojoAinda não há avaliações
- Anti Malarial DrugsDocumento107 páginasAnti Malarial DrugsSindile MchunuAinda não há avaliações
- Chemo ReceptorDocumento8 páginasChemo ReceptorCheryl Lyn SanchezAinda não há avaliações
- The Muscular SystemDocumento49 páginasThe Muscular SystemTessa Lonka TenidoAinda não há avaliações
- Unit 13 Endocrine GlandDocumento73 páginasUnit 13 Endocrine GlandChandan ShahAinda não há avaliações
- THE Circulatory SystemDocumento76 páginasTHE Circulatory SystemJerickson Javier VasquezAinda não há avaliações
- 10.neurological Assessment Cont...Documento33 páginas10.neurological Assessment Cont...Chenii RoyAinda não há avaliações
- Preoperative Preparation of Patient For SurgeryDocumento23 páginasPreoperative Preparation of Patient For SurgeryFauzi SebunyaAinda não há avaliações
- OncologyDocumento175 páginasOncologyabdurehmanAinda não há avaliações
- BSC Nursing Year 2Documento43 páginasBSC Nursing Year 2Kishan PatelAinda não há avaliações
- RESPIRATORY SYSTEM AnjuDocumento38 páginasRESPIRATORY SYSTEM Anjuanju rachel jose100% (1)
- You Are HereDocumento8 páginasYou Are HeremthanushriAinda não há avaliações
- ColostomyDocumento15 páginasColostomyJustin Ahorro-DionisioAinda não há avaliações
- Tissues: Tissue: A Tissue Is A Collection of Cells Having Similar Origin, Structure, and FunctionDocumento13 páginasTissues: Tissue: A Tissue Is A Collection of Cells Having Similar Origin, Structure, and FunctionnagahushanamAinda não há avaliações
- Lymph SystemDocumento7 páginasLymph SystemghaiathAinda não há avaliações
- Theoretical Foundation of Nursing - Florence NightingaleDocumento9 páginasTheoretical Foundation of Nursing - Florence NightingaleAshley Nicole BeltranAinda não há avaliações
- CLM.20 Microbiology Specimen CollectionDocumento19 páginasCLM.20 Microbiology Specimen Collectionfldos universeAinda não há avaliações
- Ana Phisio Lab Report.Documento4 páginasAna Phisio Lab Report.Diana Amor100% (1)
- Female External GenitaliaDocumento9 páginasFemale External Genitaliabuhari rabiuAinda não há avaliações
- Assessment of Neurological SystemDocumento26 páginasAssessment of Neurological SystemBatiao Camille Claire100% (1)
- COPDDocumento15 páginasCOPDUmapreethi Kumar100% (1)
- Muscle Strength TestingDocumento3 páginasMuscle Strength TestingGiselle Chloe Baluya ico100% (1)
- Human Anatomy,: First Edition Mckinley & O'LoughlinDocumento40 páginasHuman Anatomy,: First Edition Mckinley & O'LoughlinAgung PurmanaAinda não há avaliações
- The Human Renal SystemDocumento15 páginasThe Human Renal SystemChuche SustentoAinda não há avaliações
- Anatomy of Respiratory SystemDocumento9 páginasAnatomy of Respiratory SystemLatifah Husna Zulkafli100% (1)
- Poisoning DecontaminationDocumento14 páginasPoisoning DecontaminationadystiAinda não há avaliações
- Anatomy of The Urinary SystemDocumento24 páginasAnatomy of The Urinary Systemgaylmm100% (2)
- Ostomy Care: Esther Hattler, BS, RN, WCCDocumento51 páginasOstomy Care: Esther Hattler, BS, RN, WCCAnita TermasAinda não há avaliações
- The Human Nervous Syste1Documento10 páginasThe Human Nervous Syste1taytay321Ainda não há avaliações
- The Digestive System: Chapter 23 - Lecture NotesDocumento77 páginasThe Digestive System: Chapter 23 - Lecture NotesJonalyn ChewacheoAinda não há avaliações
- Fluid and Electrolyte Imbalance and Nutritional ProblemDocumento98 páginasFluid and Electrolyte Imbalance and Nutritional ProblemPaul EbenezerAinda não há avaliações
- Common Bile Duct (CBD) Stone (Choledocholithiasis)Documento4 páginasCommon Bile Duct (CBD) Stone (Choledocholithiasis)Manurun Londong AlloAinda não há avaliações
- Endocrine System 2017Documento28 páginasEndocrine System 2017cyber sec100% (1)
- Mantoux Test and Its Interpretation: Review ArticleDocumento5 páginasMantoux Test and Its Interpretation: Review ArticlePramudya YopalikaAinda não há avaliações
- TBDocumento5 páginasTBQuezon D. Lerog Jr.Ainda não há avaliações
- Mantoux TestDocumento3 páginasMantoux Testfarrukhhussain2006Ainda não há avaliações
- Ped Med HandbookDocumento27 páginasPed Med HandbookSoad Shedeed0% (1)
- Prospectus PgiDocumento21 páginasProspectus PgiGurmeet SinghAinda não há avaliações
- Metastaticprostatecancer 140513161922 Phpapp01 PDFDocumento37 páginasMetastaticprostatecancer 140513161922 Phpapp01 PDFGurmeet SinghAinda não há avaliações
- Secondary Puj ObstructionDocumento22 páginasSecondary Puj ObstructionGurmeet SinghAinda não há avaliações
- Robotic SurgeryDocumento6 páginasRobotic SurgeryGurmeet SinghAinda não há avaliações
- Metastaticprostatecancer 140513161922 Phpapp01 PDFDocumento37 páginasMetastaticprostatecancer 140513161922 Phpapp01 PDFGurmeet SinghAinda não há avaliações
- Prospectus December RA Updated 25april2016Documento16 páginasProspectus December RA Updated 25april2016Gurmeet SinghAinda não há avaliações
- Pediatric Surgery HandbookDocumento75 páginasPediatric Surgery HandbookAlex Vătau100% (2)
- Important Sections in Ipc, CR PC, and Iea Injuries RelatedDocumento10 páginasImportant Sections in Ipc, CR PC, and Iea Injuries Relatedkrishcute3Ainda não há avaliações
- Forensic Medicine FINAL REVISIONDocumento33 páginasForensic Medicine FINAL REVISIONjspradeepscribdAinda não há avaliações
- DAMS MicrobiologyDocumento5 páginasDAMS MicrobiologyGurmeet SinghAinda não há avaliações
- THOA-1994 Organ Sharing Act IndiaDocumento13 páginasTHOA-1994 Organ Sharing Act IndiaLibin ThathappillyAinda não há avaliações
- My Co PlasmasDocumento7 páginasMy Co PlasmasGurmeet SinghAinda não há avaliações
- Poisons: PoisonDocumento21 páginasPoisons: PoisonGurmeet SinghAinda não há avaliações
- Clinical Biochemistry ReviewDocumento10 páginasClinical Biochemistry Reviewyaykatai100% (2)
- Forensic MedicineDocumento12 páginasForensic MedicineGurmeet SinghAinda não há avaliações
- Hand Hygiene CoreDocumento27 páginasHand Hygiene CoretyasAinda não há avaliações
- Hand Hygiene CoreDocumento27 páginasHand Hygiene CoretyasAinda não há avaliações
- Drug Interaction2eDocumento69 páginasDrug Interaction2eapi-3745953Ainda não há avaliações
- Ipc Sections...Documento9 páginasIpc Sections...Gurmeet SinghAinda não há avaliações
- IMA CGP ProspectusDocumento28 páginasIMA CGP ProspectusGurmeet SinghAinda não há avaliações
- Swine Flu AlertDocumento19 páginasSwine Flu AlertGurmeet SinghAinda não há avaliações
- Mnemonic Lysosomal Storage Disorders....Documento3 páginasMnemonic Lysosomal Storage Disorders....Gurmeet Singh100% (1)
- CD MarkersDocumento4 páginasCD MarkersGurmeet SinghAinda não há avaliações
- How To Administer Injections 123Documento37 páginasHow To Administer Injections 123Gurmeet Singh100% (1)
- Infectious MyositisDocumento7 páginasInfectious MyositisGurmeet SinghAinda não há avaliações
- Diabetic Foot Disorders A Clinical Practice GuidelineDocumento14 páginasDiabetic Foot Disorders A Clinical Practice GuidelineGurmeet SinghAinda não há avaliações
- The Acute Abdomen: The Role of The Plain Film Abdominal Series MI Zucker, MDDocumento101 páginasThe Acute Abdomen: The Role of The Plain Film Abdominal Series MI Zucker, MDnazilmailAinda não há avaliações
- Sudip Praposal - 1Documento20 páginasSudip Praposal - 1Usha BbattaAinda não há avaliações
- Recycling Mind MapDocumento2 páginasRecycling Mind Mapmsole124100% (1)
- Biomediacal Waste Project FinalDocumento43 páginasBiomediacal Waste Project Finalashoknr100% (1)
- Aluminium Alloy - Wikipedia, The Free EncyclopediaDocumento12 páginasAluminium Alloy - Wikipedia, The Free EncyclopediaAshishJoshi100% (1)
- Ask A Monk EnlightenmentDocumento16 páginasAsk A Monk EnlightenmentPetruoka EdmundasAinda não há avaliações
- Nicholas Hudson - From Nation To Race: The Origin of Racial Classification in Eighteenth-CenturyDocumento19 páginasNicholas Hudson - From Nation To Race: The Origin of Racial Classification in Eighteenth-CenturyPedro IIAinda não há avaliações
- Rac Question PaperDocumento84 páginasRac Question PaperibrahimAinda não há avaliações
- Germania Agenturinfo enDocumento4 páginasGermania Agenturinfo enДушан СтепановићAinda não há avaliações
- Class 12 Maths Project On Prime NumbersDocumento13 páginasClass 12 Maths Project On Prime Numbersanon_3835245630% (1)
- Present Simple TaskDocumento3 páginasPresent Simple TaskMaria AlejandraAinda não há avaliações
- Fama Fraternitatis Rosae Crucis PDFDocumento2 páginasFama Fraternitatis Rosae Crucis PDFJudy50% (2)
- Milviz F-15e Poh V 2Documento499 páginasMilviz F-15e Poh V 2Jose Ramon Martinez GutierrezAinda não há avaliações
- Abnormalities of Placenta, Amniotic Fluid and Cord: Prepared By, B. Ezhilarasi, Nursing TutorDocumento21 páginasAbnormalities of Placenta, Amniotic Fluid and Cord: Prepared By, B. Ezhilarasi, Nursing TutorGopala KrishnanAinda não há avaliações
- Viscous Fluid Flow Frank M White Third Edition - Compress PDFDocumento4 páginasViscous Fluid Flow Frank M White Third Edition - Compress PDFDenielAinda não há avaliações
- ST 36Documento4 páginasST 36ray72roAinda não há avaliações
- Modern Myth and Magical Face Shifting Technology in Girish Karnad Hayavadana and NagamandalaDocumento2 páginasModern Myth and Magical Face Shifting Technology in Girish Karnad Hayavadana and NagamandalaKumar KumarAinda não há avaliações
- Leadership Games and ActivitiesDocumento38 páginasLeadership Games and ActivitiesWilliam Oliss100% (1)
- Ventricular Septal DefectDocumento9 páginasVentricular Septal DefectpepotchAinda não há avaliações
- SAT Biochar Ethylene Poster 10 - 10b PDFDocumento1 páginaSAT Biochar Ethylene Poster 10 - 10b PDFsherifalharamAinda não há avaliações
- Method Statement For Cable Trays & Cable Ladders InstallationDocumento7 páginasMethod Statement For Cable Trays & Cable Ladders InstallationJamal Budeiri0% (1)
- Table 1 Minimum Separation DistancesDocumento123 páginasTable 1 Minimum Separation DistancesjhonAinda não há avaliações
- IPC's 2 Edition of Guidance Manual For Herbs and Herbal Products Monographs ReleasedDocumento1 páginaIPC's 2 Edition of Guidance Manual For Herbs and Herbal Products Monographs ReleasedRakshaAinda não há avaliações
- (Eng) Zx890lch 5a Ks En316Documento13 páginas(Eng) Zx890lch 5a Ks En316MC TAK LEEAinda não há avaliações
- Shell Gadus: Designed To Do More. Just Like Our Greases - Shell GadusDocumento2 páginasShell Gadus: Designed To Do More. Just Like Our Greases - Shell Gadusperi irawanAinda não há avaliações
- 4 5803133100506483687Documento245 páginas4 5803133100506483687Malik HamidAinda não há avaliações
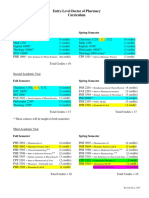
- Pharmd CurriculumDocumento18 páginasPharmd Curriculum5377773Ainda não há avaliações
- How To Eat WellDocumento68 páginasHow To Eat WelleledidiAinda não há avaliações
- Design Documentation ChecklistDocumento8 páginasDesign Documentation ChecklistGlenn Stanton100% (1)
- ME 352 Design of Machine Elements: Lab ReportDocumento5 páginasME 352 Design of Machine Elements: Lab ReportKeshav VermaAinda não há avaliações
- Binder 3 of 4 Dec-2018Documento1.169 páginasBinder 3 of 4 Dec-2018Anonymous OEmUQuAinda não há avaliações
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNo EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNota: 5 de 5 estrelas5/5 (80)
- The Obesity Code: Unlocking the Secrets of Weight LossNo EverandThe Obesity Code: Unlocking the Secrets of Weight LossNota: 4 de 5 estrelas4/5 (6)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDNo EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDNota: 5 de 5 estrelas5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNota: 2 de 5 estrelas2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityNo EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityNota: 4 de 5 estrelas4/5 (24)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNo EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNota: 4 de 5 estrelas4/5 (404)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisNo EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisNota: 4.5 de 5 estrelas4.5/5 (42)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNo EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNota: 5 de 5 estrelas5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNo EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNota: 4.5 de 5 estrelas4.5/5 (266)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisNo EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisNota: 4 de 5 estrelas4/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsAinda não há avaliações
- Why We Die: The New Science of Aging and the Quest for ImmortalityNo EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityNota: 4 de 5 estrelas4/5 (3)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryNo EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryNota: 4 de 5 estrelas4/5 (44)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.No EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Nota: 4.5 de 5 estrelas4.5/5 (110)
- Gut: the new and revised Sunday Times bestsellerNo EverandGut: the new and revised Sunday Times bestsellerNota: 4 de 5 estrelas4/5 (392)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisNo EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisNota: 3.5 de 5 estrelas3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNo EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNota: 3.5 de 5 estrelas3.5/5 (3)
- The Marshmallow Test: Mastering Self-ControlNo EverandThe Marshmallow Test: Mastering Self-ControlNota: 4.5 de 5 estrelas4.5/5 (58)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingNo EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingNota: 4 de 5 estrelas4/5 (1138)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningNo EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningNota: 4 de 5 estrelas4/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsNo EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsNota: 4.5 de 5 estrelas4.5/5 (169)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessNo EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessNota: 4.5 de 5 estrelas4.5/5 (328)
- A Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsNo EverandA Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsNota: 4.5 de 5 estrelas4.5/5 (6)