Você também pode gostar
- Gandanta and SandhiDocumento10 páginasGandanta and Sandhiambasyapare1Ainda não há avaliações
- Bond Risk A Theory of Relativity Vanguard BlogDocumento4 páginasBond Risk A Theory of Relativity Vanguard Blogambasyapare1Ainda não há avaliações
- Callan Periodoc Table of Investment ReturnsDocumento2 páginasCallan Periodoc Table of Investment Returnsambasyapare1Ainda não há avaliações
- Bonds Can Help Stock Investors Monitor Correction Risk - Seeking AlphaDocumento7 páginasBonds Can Help Stock Investors Monitor Correction Risk - Seeking Alphaambasyapare1Ainda não há avaliações
- Budget Worksheet: Monthly AmountDocumento2 páginasBudget Worksheet: Monthly Amountambasyapare1Ainda não há avaliações
- Best Way To Sell A Gold CoinDocumento16 páginasBest Way To Sell A Gold Coinambasyapare1Ainda não há avaliações
- # A B C D E F G H I J K L M N O P Q R S T U V W X: Membership Home Portfolio Stocks Bonds Funds Etfs Cefs Markets ToolsDocumento2 páginas# A B C D E F G H I J K L M N O P Q R S T U V W X: Membership Home Portfolio Stocks Bonds Funds Etfs Cefs Markets Toolsambasyapare1Ainda não há avaliações
- Bond Risk A Theory of Relativity Vanguard BlogDocumento4 páginasBond Risk A Theory of Relativity Vanguard Blogambasyapare1Ainda não há avaliações
- Bibliography - Using A Deferred Annuity To Fund A Qualified Retirement Plan - Industry ViewDocumento12 páginasBibliography - Using A Deferred Annuity To Fund A Qualified Retirement Plan - Industry Viewambasyapare1Ainda não há avaliações
- Bermstein and Stocks Efficient FrontierDocumento3 páginasBermstein and Stocks Efficient Frontierambasyapare1Ainda não há avaliações
- APMEX - Buying Precious MetalsDocumento18 páginasAPMEX - Buying Precious Metalsambasyapare1Ainda não há avaliações
- Arnott Why Cap-Weighted Indexing Is FlawedDocumento21 páginasArnott Why Cap-Weighted Indexing Is Flawedambasyapare1Ainda não há avaliações
- Benchmark Buyback MoatDocumento3 páginasBenchmark Buyback Moatambasyapare1Ainda não há avaliações
- Beginner Mistakes: How To Avoid ThemDocumento8 páginasBeginner Mistakes: How To Avoid Themambasyapare1Ainda não há avaliações
- Attorney General Michigan - Annuities Are They The Right Investment For MeDocumento4 páginasAttorney General Michigan - Annuities Are They The Right Investment For Meambasyapare1Ainda não há avaliações
- Avoiding S Corporation I.E.D.'s - Presentation SlidesDocumento33 páginasAvoiding S Corporation I.E.D.'s - Presentation Slidesambasyapare1Ainda não há avaliações
- Annuities: Ection NtroductionDocumento12 páginasAnnuities: Ection Ntroductionambasyapare1Ainda não há avaliações
- Are Bonds Adding To Your Equity ExposureDocumento4 páginasAre Bonds Adding To Your Equity Exposureambasyapare1Ainda não há avaliações
- About That Rigging ClaimDocumento3 páginasAbout That Rigging Claimambasyapare1Ainda não há avaliações
- A Look at 401 (K) Plan Fees US DPT of LaborDocumento8 páginasA Look at 401 (K) Plan Fees US DPT of Laborambasyapare1Ainda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Art 16-18Documento528 páginasArt 16-18ErudíhenAinda não há avaliações
- r315 Quick Start PDFDocumento80 páginasr315 Quick Start PDFfdsfasdsfadsAinda não há avaliações
- Air Quality Index Analysis & PredictionDocumento34 páginasAir Quality Index Analysis & PredictionGottumukkala Sravan KumarAinda não há avaliações
- MCQ Unit 3Documento15 páginasMCQ Unit 3gaur1234Ainda não há avaliações
- 6.m.tech-Ece-Vlsi, Vlsi Systems, Vlsi System Design (Vlsi, Vlsis, Vlsisd) r17 Course Structure & SyllabiDocumento35 páginas6.m.tech-Ece-Vlsi, Vlsi Systems, Vlsi System Design (Vlsi, Vlsis, Vlsisd) r17 Course Structure & SyllabiravibabukancharlaAinda não há avaliações
- Asms 02 0033Documento6 páginasAsms 02 0033Delfia AkiharyAinda não há avaliações
- Psychological Factors Influencing Technology Adoption A Case S - 2021 - TechnovDocumento17 páginasPsychological Factors Influencing Technology Adoption A Case S - 2021 - Technov6helmi6nauval6Ainda não há avaliações
- The Heart: Dr. Silvia BoyajianDocumento44 páginasThe Heart: Dr. Silvia BoyajianAsem YousefAinda não há avaliações
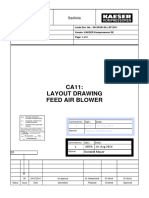
- Layout - Foundation Drawing - Air BlowerDocumento2 páginasLayout - Foundation Drawing - Air BlowerBabel THIAMAinda não há avaliações
- ClassnotesonbasicDC DCconverters EP N4Documento23 páginasClassnotesonbasicDC DCconverters EP N4Gerardo Treviño GarciaAinda não há avaliações
- Bendable ConcreteDocumento21 páginasBendable ConcreteJulia Sebastian0% (1)
- Gurps Fallout HandgunsDocumento1 páginaGurps Fallout HandgunsAndrew Scott100% (1)
- Flares & VentsDocumento29 páginasFlares & VentsSonu Kaka KakaAinda não há avaliações
- Vet CareplanexampleDocumento6 páginasVet CareplanexampleAnonymous eJZ5HcAinda não há avaliações
- Zen Intro To Buddhism & Practice of ZazenDocumento33 páginasZen Intro To Buddhism & Practice of ZazendudcomeonAinda não há avaliações
- Std9thMathsBridgeCourse (4) (001-040) .MR - enDocumento40 páginasStd9thMathsBridgeCourse (4) (001-040) .MR - ensilent gamerAinda não há avaliações
- PGC Inquiries Chapter 7 Grid ProtectionDocumento7 páginasPGC Inquiries Chapter 7 Grid ProtectionhansamvAinda não há avaliações
- Cryogenic Insulation TechnologyDocumento61 páginasCryogenic Insulation Technologyeduard.turon100% (1)
- Geo-Technical Investigation On Black Cotton Soils: GeotechnicalinvestigationonblackcottonsoilsDocumento5 páginasGeo-Technical Investigation On Black Cotton Soils: GeotechnicalinvestigationonblackcottonsoilsDevendrasinh PadhiyarAinda não há avaliações
- My Ideal Home: Name No. Class Date Mark TeacherDocumento5 páginasMy Ideal Home: Name No. Class Date Mark TeacherQuadrado MágicoAinda não há avaliações
- Primbon Command 3GDocumento3 páginasPrimbon Command 3GEriska FebriantoAinda não há avaliações
- Growth Rate and Fattening Potetial of Meat AnimalsDocumento54 páginasGrowth Rate and Fattening Potetial of Meat AnimalsMuhammad Shahzad ChandiaAinda não há avaliações
- Air Show - Blue Angels in Flying K - The News of NAS KingsvilleDocumento16 páginasAir Show - Blue Angels in Flying K - The News of NAS KingsvilleAlan GuggenheimAinda não há avaliações
- Electromagnetic and Thermal AnalysisDocumento5 páginasElectromagnetic and Thermal AnalysishamidrezaAinda não há avaliações
- Module Letter 1Documento2 páginasModule Letter 1eeroleAinda não há avaliações
- Medical BiotechnologyDocumento4 páginasMedical Biotechnologyعمر بن عليAinda não há avaliações
- 100% Chemical-Free Solution For Organic Farming: Where Health Is A HabitDocumento2 páginas100% Chemical-Free Solution For Organic Farming: Where Health Is A Habitamit4118Ainda não há avaliações
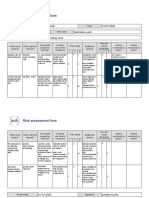
- Risk Assessment Project Iosh - MsDocumento2 páginasRisk Assessment Project Iosh - MsSanjeev Kumar75% (32)
- BookDocumento28 páginasBookFebrian Wardoyo100% (1)
- Energy and FluctuationDocumento10 páginasEnergy and Fluctuationwalid Ait MazouzAinda não há avaliações