Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Robert Miller's Feeling-State Addiction Protocol Cheat SheetDocumento1 páginaRobert Miller's Feeling-State Addiction Protocol Cheat SheetZenobia Niculita100% (1)
- Forgiveness BookletDocumento14 páginasForgiveness BookletClau SánchezAinda não há avaliações
- Hypnosis Course by Magic LeoDocumento35 páginasHypnosis Course by Magic LeoVeerasamy Puratchimani100% (2)
- Defining HypnosisDocumento6 páginasDefining HypnosisblackvenumAinda não há avaliações
- Erich Fromm, DT Suzuki, and Zen BuddhismDocumento8 páginasErich Fromm, DT Suzuki, and Zen BuddhismColumbia University Press100% (2)
- Affective Learning CompetenciesDocumento10 páginasAffective Learning CompetenciesMarry DanielAinda não há avaliações
- MpiDocumento7 páginasMpiVipin Yadav100% (1)
- Tattwa Work - Mad - AbeDocumento2 páginasTattwa Work - Mad - AbeJosé Roberto Romeiro Abrahão100% (4)
- Key Points On TrekchöDocumento3 páginasKey Points On TrekchöChris Christodoulidis100% (1)
- Google's Project Oxygen - Do Managers MatterDocumento9 páginasGoogle's Project Oxygen - Do Managers MatterbukhariAinda não há avaliações
- Operant ConditioningDocumento14 páginasOperant Conditioningniks2409Ainda não há avaliações
- Yelurban Hotel and RestaurantDocumento2 páginasYelurban Hotel and RestaurantDonamir CatorAinda não há avaliações
- Meditation Techniques for Inner Peace and Self-RealizationDocumento2 páginasMeditation Techniques for Inner Peace and Self-Realizationpradip2190Ainda não há avaliações
- Stress and Nishkama Karma Dr. Shriniwas KashalikarDocumento3 páginasStress and Nishkama Karma Dr. Shriniwas KashalikarShriniwas Janardan KashalikarAinda não há avaliações
- Assingment On IGBODocumento15 páginasAssingment On IGBOaartiAinda não há avaliações
- Appendix 1 Emotional Intelligence QuestionnaireDocumento7 páginasAppendix 1 Emotional Intelligence QuestionnaireDivya ThomasAinda não há avaliações
- Reflective JournalDocumento12 páginasReflective JournalMuhammad Sajid SaeedAinda não há avaliações
- Coping With Stress and Anxiety PDFDocumento79 páginasCoping With Stress and Anxiety PDFmihalel100% (1)
- Lonnie Athens' 4-stage process of violentizationDocumento18 páginasLonnie Athens' 4-stage process of violentizationJUAN CARLOS TORRES CORREAAinda não há avaliações
- The Aesthetics of Silence / Susan Sontag: DuchampDocumento12 páginasThe Aesthetics of Silence / Susan Sontag: DuchampmonicanuAinda não há avaliações
- g3 - ArticleDocumento6 páginasg3 - Articleapi-405035830Ainda não há avaliações
- (Singh, R. Raj. Schopenhauer: A Guide For The Perplexed. Bloomsbury Publishing, 2010Documento13 páginas(Singh, R. Raj. Schopenhauer: A Guide For The Perplexed. Bloomsbury Publishing, 2010Yajat BhargavAinda não há avaliações
- PerdevDocumento11 páginasPerdevrosemarie paleAinda não há avaliações
- Creativiaty, Expressivity And, Yoga in Motion - The Five EXPs Workshops Manual (Unfinished Draft Version)Documento61 páginasCreativiaty, Expressivity And, Yoga in Motion - The Five EXPs Workshops Manual (Unfinished Draft Version)Giuseppe RosatoAinda não há avaliações
- OPINIONSDocumento27 páginasOPINIONSRose DanielleAinda não há avaliações
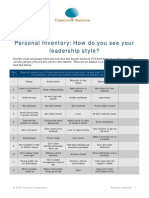
- Personal Inventory: How Do You See Your Leadership Style?Documento9 páginasPersonal Inventory: How Do You See Your Leadership Style?VinceWijayaAinda não há avaliações
- Master Your EmotionsDocumento16 páginasMaster Your EmotionsJosh NobinsAinda não há avaliações
- Schlossbergs Theory SlidesDocumento20 páginasSchlossbergs Theory Slidesapi-327238966100% (1)
- Discuss Two Errors in AttributionsDocumento3 páginasDiscuss Two Errors in AttributionsJack ChonAinda não há avaliações
- Epistemological Dualism Vs Metaphysical DualismDocumento13 páginasEpistemological Dualism Vs Metaphysical DualismJohn Moore Jr.Ainda não há avaliações