Você também pode gostar
- Stages of ChangeDocumento3 páginasStages of Changeelvinegunawan100% (1)
- Locke-Wallace Short Marital-Adjustment TestDocumento16 páginasLocke-Wallace Short Marital-Adjustment TestelvinegunawanAinda não há avaliações
- Classification of Sleep DisordersDocumento15 páginasClassification of Sleep Disorderselvinegunawan100% (1)
- Classification of Sleep DisordersDocumento15 páginasClassification of Sleep Disorderselvinegunawan100% (1)
- The Reliability of Relationship SatisfactionDocumento10 páginasThe Reliability of Relationship SatisfactionelvinegunawanAinda não há avaliações
- The Influence of Personality On Adherence To Methadone Maintenance Treatment in Methadone Clinic in Hasan Sadikin General HospitalDocumento1 páginaThe Influence of Personality On Adherence To Methadone Maintenance Treatment in Methadone Clinic in Hasan Sadikin General HospitalelvinegunawanAinda não há avaliações
- Early Marriage A Root of Current Physiological and Psychosocial Health BurdensDocumento4 páginasEarly Marriage A Root of Current Physiological and Psychosocial Health BurdenselvinegunawanAinda não há avaliações
- Duration of Untreated Psychosis and The Long-Term Course of SchizophreniaDocumento4 páginasDuration of Untreated Psychosis and The Long-Term Course of SchizophreniaelvinegunawanAinda não há avaliações
- BFI ScoringDocumento2 páginasBFI ScoringelvinegunawanAinda não há avaliações
- Report of Drug S TestingDocumento2 páginasReport of Drug S TestingelvinegunawanAinda não há avaliações
- Form PenilaianDocumento72 páginasForm PenilaianelvinegunawanAinda não há avaliações
- Medical Student AwardsDocumento1 páginaMedical Student AwardselvinegunawanAinda não há avaliações
- APA SAMHSA Minority FellowshipDocumento1 páginaAPA SAMHSA Minority FellowshipelvinegunawanAinda não há avaliações
- Letter of Intent: Board Certified Non Board Certified Board Eligible (Date of Scheduled Exam) Individual: GroupDocumento2 páginasLetter of Intent: Board Certified Non Board Certified Board Eligible (Date of Scheduled Exam) Individual: GroupelvinegunawanAinda não há avaliações
- Duration of Untreated Psychosis and Negative Symptoms - A Systematic Review and Meta-Analysis of Individual Patient DataDocumento22 páginasDuration of Untreated Psychosis and Negative Symptoms - A Systematic Review and Meta-Analysis of Individual Patient DataelvinegunawanAinda não há avaliações
- Untreated Initial Psychosis: Relation To Cognitive Deficits and Brain Morphology in First-Episode SchizophreniaDocumento7 páginasUntreated Initial Psychosis: Relation To Cognitive Deficits and Brain Morphology in First-Episode SchizophreniaelvinegunawanAinda não há avaliações
- Clinical Neuropsychiatry (2008) 5, 6, 263-272: S J 2008, A F 2009Documento10 páginasClinical Neuropsychiatry (2008) 5, 6, 263-272: S J 2008, A F 2009elvinegunawanAinda não há avaliações
- Schizophrenia Research: For The JAST Study GroupDocumento10 páginasSchizophrenia Research: For The JAST Study GroupelvinegunawanAinda não há avaliações
- Clinical Psychopathology PDFDocumento5 páginasClinical Psychopathology PDFelvinegunawan50% (2)
- The Brief Assessment of Cognition in Affective Disorders (Bac-A) : A New Instrument For Assessing Cognitive Functioning in Bipolar DisorderDocumento1 páginaThe Brief Assessment of Cognition in Affective Disorders (Bac-A) : A New Instrument For Assessing Cognitive Functioning in Bipolar DisorderelvinegunawanAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Compile Nclex - RN Questions and AnswersDocumento17 páginasCompile Nclex - RN Questions and Answerseric0% (1)
- PPTDocumento28 páginasPPTuculucullAinda não há avaliações
- Maduna 2006 The Role of Traditional Medicine in The Treatment of Diabetes MellitusDocumento4 páginasMaduna 2006 The Role of Traditional Medicine in The Treatment of Diabetes MellitusMiksAinda não há avaliações
- Chemical and Nutritional Compositions of Flame of Forest (Delonix Regia) Seeds and Seed OilDocumento5 páginasChemical and Nutritional Compositions of Flame of Forest (Delonix Regia) Seeds and Seed OilAbdulrasaq OyedejiAinda não há avaliações
- PlenaryDocumento31 páginasPlenaryIsmail AbdullahAinda não há avaliações
- UNIVERSITY OF MEDICAL SCIENCES"REZONANCA"-Halil Ajvazi/Ophthalmology/Prishtina/Republic of KosovaDocumento98 páginasUNIVERSITY OF MEDICAL SCIENCES"REZONANCA"-Halil Ajvazi/Ophthalmology/Prishtina/Republic of KosovaHALIL Z.AJVAZI100% (1)
- Jurnal MalabsorbsiDocumento6 páginasJurnal MalabsorbsiIda Putri IhsaniAinda não há avaliações
- Age ( 55 Years Old) - Female Sex - BMI: 28 (Overweight) - Alcohol Consumption - Uncontrolled Hypertension - High Fat DietDocumento3 páginasAge ( 55 Years Old) - Female Sex - BMI: 28 (Overweight) - Alcohol Consumption - Uncontrolled Hypertension - High Fat DietelleAinda não há avaliações
- HEATS ManualDocumento66 páginasHEATS ManualFitri SyawalAinda não há avaliações
- DS Clarithromycin GI ARLEDDocumento5 páginasDS Clarithromycin GI ARLEDvivi's eyebrowsAinda não há avaliações
- PedigreesDocumento5 páginasPedigreestpn72hjg88Ainda não há avaliações
- Causes of BronchopneumoniaDocumento6 páginasCauses of BronchopneumoniaSuhas Ingale100% (1)
- Assignment On Health Assessment 1Documento5 páginasAssignment On Health Assessment 1Sumit YadavAinda não há avaliações
- Guidelines For Preventing Foodborne Illness in SchoolDocumento27 páginasGuidelines For Preventing Foodborne Illness in Schoolnaveed_akbar_2Ainda não há avaliações
- tmpBC74 TMPDocumento7 páginastmpBC74 TMPFrontiersAinda não há avaliações
- STS100 - That SugarDocumento3 páginasSTS100 - That Sugarbjornebol01Ainda não há avaliações
- Good Escort Guide With SW5 CorrectionsDocumento12 páginasGood Escort Guide With SW5 CorrectionsNaveen DagarAinda não há avaliações
- Journal GastroenterologyDocumento14 páginasJournal GastroenterologySusilo PrihrantoAinda não há avaliações
- Nutrition 1Documento5 páginasNutrition 1Christine PunsalanAinda não há avaliações
- Reading ComprehensionDocumento6 páginasReading ComprehensionJacques Robert0% (3)
- The Mental Status ExamDocumento3 páginasThe Mental Status ExamShrests SinhaAinda não há avaliações
- Family Planning Association of India Madurai BranchDocumento12 páginasFamily Planning Association of India Madurai BranchValarmathiAinda não há avaliações
- HypotrophyDocumento3 páginasHypotrophyopeyemi daramolaAinda não há avaliações
- Murach Bagley - 2016 - Skeletal Muscle Hypertrophy With Concurrent Exercise TrainingDocumento11 páginasMurach Bagley - 2016 - Skeletal Muscle Hypertrophy With Concurrent Exercise TrainingMarko BrzakAinda não há avaliações
- Charcot-Marie-Tooth DiseaseDocumento2 páginasCharcot-Marie-Tooth DiseaseitsmeayaeAinda não há avaliações
- Hypertensive Retinopathy - Yanoff and DukerDocumento13 páginasHypertensive Retinopathy - Yanoff and DukerriveliAinda não há avaliações
- Carpal Tunnel SyndromeDocumento43 páginasCarpal Tunnel SyndromePra YudhaAinda não há avaliações
- Malaria: Dr. Harun Hudari, SPPDDocumento49 páginasMalaria: Dr. Harun Hudari, SPPDEdvans HenryAinda não há avaliações
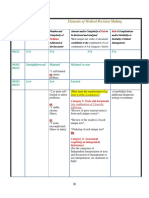
- 3-Level of MDMDocumento3 páginas3-Level of MDMmedical codingAinda não há avaliações
- Genetic Disorders: John W. BachmanDocumento19 páginasGenetic Disorders: John W. BachmannehaAinda não há avaliações