Você também pode gostar
- PHPQ 6 X 8 SSDocumento6 páginasPHPQ 6 X 8 SSprecillathoppilAinda não há avaliações
- AbgDocumento8 páginasAbgprecillathoppilAinda não há avaliações
- Injections: Subcutaneous Intramuscular MedicationsDocumento9 páginasInjections: Subcutaneous Intramuscular MedicationsprecillathoppilAinda não há avaliações
- Visit To Nariniketan Jabalpur: 1. To Encourages Adoption of Orphans and Destitute Children. 2. 3. 4. 5. 6. 7Documento7 páginasVisit To Nariniketan Jabalpur: 1. To Encourages Adoption of Orphans and Destitute Children. 2. 3. 4. 5. 6. 7precillathoppilAinda não há avaliações
- Master Rotatoin Plan M.SC Nursing 1st YearDocumento2 páginasMaster Rotatoin Plan M.SC Nursing 1st YearprecillathoppilAinda não há avaliações
- Current Trends in Nursing Educaion..MadhuDocumento13 páginasCurrent Trends in Nursing Educaion..Madhuprecillathoppil100% (1)
- Course PlANDocumento7 páginasCourse PlANprecillathoppil50% (4)
- Principles of PreventionDocumento14 páginasPrinciples of PreventionprecillathoppilAinda não há avaliações
- Models of PreventionDocumento21 páginasModels of Preventionprecillathoppil100% (5)
- Av Aids FinalDocumento17 páginasAv Aids Finalprecillathoppil0% (1)
- Guidance & CounsellingDocumento16 páginasGuidance & Counsellingprecillathoppil75% (8)
- HydrocephalusDocumento21 páginasHydrocephalusprecillathoppil100% (2)
- CURRENT STATUS OF CHILD HEALTH IN INDIA To Be PrintDocumento6 páginasCURRENT STATUS OF CHILD HEALTH IN INDIA To Be Printprecillathoppil96% (24)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Full Download Human Memory 2nd Radvansky Test Bank PDF Full ChapterDocumento36 páginasFull Download Human Memory 2nd Radvansky Test Bank PDF Full Chaptersugarysestine.fllo5z100% (18)
- Emotion in HumanisticDocumento32 páginasEmotion in HumanisticpsicandreiaAinda não há avaliações
- Listening Skills Practice: The Fear Factor - Exercises: PreparationDocumento3 páginasListening Skills Practice: The Fear Factor - Exercises: PreparationRomina ManesAinda não há avaliações
- Dreams, Embodied Imagination and The Creative Mind: A Pilot StudyDocumento17 páginasDreams, Embodied Imagination and The Creative Mind: A Pilot StudyLisandro MartinAinda não há avaliações
- Management of Peripheral Neuropathy With B1 B6 and B12 - Dr. Oscar Nurhadi, Sp. SDocumento52 páginasManagement of Peripheral Neuropathy With B1 B6 and B12 - Dr. Oscar Nurhadi, Sp. SMuhammad FirdaudAinda não há avaliações
- Dopamine HypothesisDocumento2 páginasDopamine HypothesisBo123456100% (3)
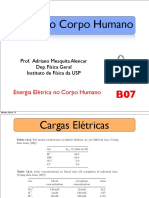
- Física Do Corpo Humano: Prof. Adriano Mesquita Alencar Dep. Física Geral Instituto de Física Da USPDocumento31 páginasFísica Do Corpo Humano: Prof. Adriano Mesquita Alencar Dep. Física Geral Instituto de Física Da USPMariaSuzanaDiazAinda não há avaliações
- Science Grade 3 LAS FnalDocumento13 páginasScience Grade 3 LAS FnalSan Isidro ISAinda não há avaliações
- From Stimulus To Symbol: The Economy of Biological Computation (Von Foerster)Documento15 páginasFrom Stimulus To Symbol: The Economy of Biological Computation (Von Foerster)telecult100% (3)
- Multiple Disability Original HandoutDocumento42 páginasMultiple Disability Original HandoutHabtamu DebasuAinda não há avaliações
- MedvizzDocumento1 páginaMedvizzSaeda AhmedAinda não há avaliações
- Memoria Autobiografica Suntem Dependenti de Trecut?: Dragos Cirneci Universitatea Spiru Haret BucurestiDocumento53 páginasMemoria Autobiografica Suntem Dependenti de Trecut?: Dragos Cirneci Universitatea Spiru Haret Bucurestiflorina eAinda não há avaliações
- Science6 Qtr2 Set1-FinalDocumento32 páginasScience6 Qtr2 Set1-FinalLady Jae ArbesoAinda não há avaliações
- Electroencephalography in Pediatric EpilepsyDocumento12 páginasElectroencephalography in Pediatric EpilepsyPrankur PandeyAinda não há avaliações
- Nervous SystemDocumento12 páginasNervous SystemLeon MarkoAinda não há avaliações
- 19A Glutamate, Glycine, & GABADocumento23 páginas19A Glutamate, Glycine, & GABAGe NavAinda não há avaliações
- 104 - Neurology Physiology) Spinal Cord - Golgi Tendon Organ Reflex (GTO)Documento3 páginas104 - Neurology Physiology) Spinal Cord - Golgi Tendon Organ Reflex (GTO)Nikki Lin LiuAinda não há avaliações
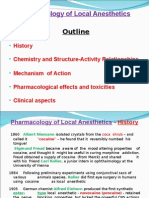
- Pharmacology of Local AnestheticsDocumento32 páginasPharmacology of Local AnestheticsJk FloresAinda não há avaliações
- Anatomy and Physiology-REVIEWER-Practical ExamDocumento12 páginasAnatomy and Physiology-REVIEWER-Practical ExamDeity Ann ReuterezAinda não há avaliações
- Osta Lecture 4 Notes Online ENGLISH Base of Skull and BrainDocumento36 páginasOsta Lecture 4 Notes Online ENGLISH Base of Skull and BrainslyfoxkittyAinda não há avaliações
- ReportDocumento31 páginasReportgunratna kambleAinda não há avaliações
- Ebook Electromyography and Neuromuscular Disorders Clinical Electrophysiologic Ultrasound Correlations PDF Full Chapter PDFDocumento68 páginasEbook Electromyography and Neuromuscular Disorders Clinical Electrophysiologic Ultrasound Correlations PDF Full Chapter PDFhelen.reid678100% (25)
- Language, Orientation, Memory, Attention Span and Calculation, LOCDocumento7 páginasLanguage, Orientation, Memory, Attention Span and Calculation, LOCYessamin Paith RoderosAinda não há avaliações
- Ratio - Neuro (VR 2.O)Documento24 páginasRatio - Neuro (VR 2.O)Accey RamirezAinda não há avaliações
- Chapter 2: Articulatory, Auditory and Acoustic Phonetics. PhonologyDocumento4 páginasChapter 2: Articulatory, Auditory and Acoustic Phonetics. PhonologycalluraAinda não há avaliações
- John Medina - Brain Rules PDFDocumento11 páginasJohn Medina - Brain Rules PDFDiego Cunha100% (2)
- Brain CancerDocumento3 páginasBrain CancerBunnie AlphaAinda não há avaliações
- Endoscopic Ear Surgery Course. 4th Edition: Barcelona, April 27, 2022Documento1 páginaEndoscopic Ear Surgery Course. 4th Edition: Barcelona, April 27, 2022Luana Maria GherasieAinda não há avaliações
- Bci ProjectDocumento3 páginasBci ProjectAndy yelweAinda não há avaliações
- MCQSDocumento25 páginasMCQSkays30002403Ainda não há avaliações