Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Adler - On Broadway - Art and Commerce On The Great White WayDocumento269 páginasAdler - On Broadway - Art and Commerce On The Great White WayCharles Davidson100% (2)
- The Visual Collaboration: Working With DesignersDocumento35 páginasThe Visual Collaboration: Working With DesignersCharles DavidsonAinda não há avaliações
- Analyzing The Script: Construction and MeaningDocumento34 páginasAnalyzing The Script: Construction and MeaningCharles DavidsonAinda não há avaliações
- Application To Direct at The Washington Community TheaterDocumento4 páginasApplication To Direct at The Washington Community TheaterCharles DavidsonAinda não há avaliações
- MGN 477 MLC Outer Cover MSF 4156Documento2 páginasMGN 477 MLC Outer Cover MSF 4156Charles DavidsonAinda não há avaliações
- MGN 477 MLC List of Crew MSF 4157Documento1 páginaMGN 477 MLC List of Crew MSF 4157Charles DavidsonAinda não há avaliações
- MGN 477 MLC List of Young Persons MSF 4158Documento2 páginasMGN 477 MLC List of Young Persons MSF 4158Charles DavidsonAinda não há avaliações
- Student Achievement Record HRBDocumento1 páginaStudent Achievement Record HRBCharles DavidsonAinda não há avaliações
- Godspell SynopsisDocumento4 páginasGodspell SynopsisCharles DavidsonAinda não há avaliações
- Uc2.ark 13960 t5t72cg70Documento563 páginasUc2.ark 13960 t5t72cg70Charles DavidsonAinda não há avaliações
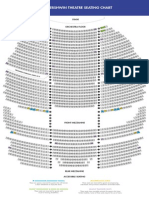
- The Gershwin Theatre Seating Chart: StageDocumento1 páginaThe Gershwin Theatre Seating Chart: StageCharles DavidsonAinda não há avaliações
- AFTR Test ParametersDocumento1 páginaAFTR Test ParametersCharles DavidsonAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Standard For The Management of Narcotics and Controlled Medicinal ProductsDocumento10 páginasStandard For The Management of Narcotics and Controlled Medicinal ProductsVhince PiscoAinda não há avaliações
- CHP Manual EN-webfinal PDFDocumento29 páginasCHP Manual EN-webfinal PDFmajaklipaAinda não há avaliações
- Patient Safety and Clinical RiskDocumento5 páginasPatient Safety and Clinical Riskshylajathomas33Ainda não há avaliações
- Courier: A Thousand WordsDocumento20 páginasCourier: A Thousand WordsAnonymous 9eadjPSJNgAinda não há avaliações
- Telemanas ProspectusDocumento29 páginasTelemanas ProspectusMehbub Hasan ChoudhuryAinda não há avaliações
- Presentation PBLM WTH ObjDocumento12 páginasPresentation PBLM WTH ObjKavi rajputAinda não há avaliações
- Nursing Program: PACUCOA, Level IV Accredited StatusDocumento9 páginasNursing Program: PACUCOA, Level IV Accredited StatusKurt RoseteAinda não há avaliações
- Community Public Health Nursing Practice Health For Families and Populations 5th Edition Maurer Test BankDocumento11 páginasCommunity Public Health Nursing Practice Health For Families and Populations 5th Edition Maurer Test BankKyla100% (2)
- The Globalization of Health Care: Digital Assignment 3Documento1 páginaThe Globalization of Health Care: Digital Assignment 3Ayeesha K.s.Ainda não há avaliações
- Betty Neuman: Systems Theory in Nursing PracticeDocumento4 páginasBetty Neuman: Systems Theory in Nursing PracticeJeremy CollamarAinda não há avaliações
- Tata Aig Medicare Premier: Policy WordingsDocumento16 páginasTata Aig Medicare Premier: Policy WordingsSiddhartha PorwalAinda não há avaliações
- RPRH Law (RA 10354) Report, 2015 (Popular Version) - Min PDFDocumento40 páginasRPRH Law (RA 10354) Report, 2015 (Popular Version) - Min PDFRuzzell AlvarezAinda não há avaliações
- What Doctors Know - Vol 1 Issue 1Documento86 páginasWhat Doctors Know - Vol 1 Issue 1What Doctors KnowAinda não há avaliações
- Antiphospholipid Antibody Syndrome The.2 PDFDocumento5 páginasAntiphospholipid Antibody Syndrome The.2 PDFJunita Nelly Esther JosephAinda não há avaliações
- Operating Room Surgical ProceduresDocumento197 páginasOperating Room Surgical ProceduresChin Chan100% (6)
- OFA Bariatric Surgery Poster Euroanesthesia 2023Documento1 páginaOFA Bariatric Surgery Poster Euroanesthesia 2023Nataša SojčićAinda não há avaliações
- FIGO Cancer Report 2018Documento2 páginasFIGO Cancer Report 2018Anonymous 2XsadJlrAinda não há avaliações
- Book Reviews: University of Charleston School of Pharmacy, Charleston, WVDocumento2 páginasBook Reviews: University of Charleston School of Pharmacy, Charleston, WVWahyuniAinda não há avaliações
- Trial of ScarDocumento12 páginasTrial of Scarnyangara50% (2)
- Role and Function of The MidwifeDocumento35 páginasRole and Function of The Midwifenessa100% (7)
- AsthmaDocumento18 páginasAsthmaKainanAinda não há avaliações
- Outpatient Clinic (Hospital Department) - WikipediaDocumento6 páginasOutpatient Clinic (Hospital Department) - WikipediaG MAinda não há avaliações
- Scale Up and Postapproval Changes (Supac) Guidance For Industry: A Regulatory NoteDocumento9 páginasScale Up and Postapproval Changes (Supac) Guidance For Industry: A Regulatory NoteAKKAD PHARMAAinda não há avaliações
- IMNCHDocumento94 páginasIMNCHAms BeeAinda não há avaliações
- Cac Ethiopia - Istanbul Tours 2022Documento6 páginasCac Ethiopia - Istanbul Tours 2022Awol AminAinda não há avaliações
- Max Medic Plan 1Documento1 páginaMax Medic Plan 1Premkumar NadarajanAinda não há avaliações
- 2009 Schedule of ExamDocumento2 páginas2009 Schedule of ExamPRC Baguio100% (13)
- Smart PumpsDocumento98 páginasSmart PumpsVictor Akira Santos SatoAinda não há avaliações
- Team 5 Project Proposal Iged392-02 Final 07aug21Documento13 páginasTeam 5 Project Proposal Iged392-02 Final 07aug21api-569020074Ainda não há avaliações
- Update: Diagnostic Statistical Manual Mental DisordersDocumento30 páginasUpdate: Diagnostic Statistical Manual Mental DisordersFebelin Idjie ElsaMomAinda não há avaliações