Você também pode gostar
- MSU-M SENIOR HIGH SCHOOL SASE REVIEW 2017 LIFE SCIENCEDocumento5 páginasMSU-M SENIOR HIGH SCHOOL SASE REVIEW 2017 LIFE SCIENCECyrel Sudaria92% (37)
- Case Study PneumoniaDocumento13 páginasCase Study Pneumonialavparedes93% (44)
- BRONCHIECTASIS: CAUSES, SYMPTOMS AND TREATMENTDocumento40 páginasBRONCHIECTASIS: CAUSES, SYMPTOMS AND TREATMENTImmanuel100% (2)
- Chronic Bronchitis in Exacerbation Cor Pulmonale With HypertensionDocumento61 páginasChronic Bronchitis in Exacerbation Cor Pulmonale With HypertensionGrace Dela Rosa Melecio50% (4)
- Glycerol Uptake Preserves Cut Juvenile Foliage of Eucalyptus CinereaDocumento11 páginasGlycerol Uptake Preserves Cut Juvenile Foliage of Eucalyptus CinereaAndreaAinda não há avaliações
- lec.1 Obstructive Lung Diseases saifDocumento23 páginaslec.1 Obstructive Lung Diseases saifs2111110520Ainda não há avaliações
- Dr. Sana Bashir DPT, MS-CPPTDocumento46 páginasDr. Sana Bashir DPT, MS-CPPTbkdfiesefll100% (1)
- Interstitial Lung DiseaseDocumento14 páginasInterstitial Lung DiseaseAzkaZulfiqarAinda não há avaliações
- PathologyDocumento159 páginasPathologyIkram ShinwariAinda não há avaliações
- 12.lung PathologyDocumento4 páginas12.lung PathologyMuhammad Zarak NiaziAinda não há avaliações
- I Lower Respiratory System PathologyDocumento12 páginasI Lower Respiratory System PathologyBaha Al AdaylehAinda não há avaliações
- Broncho PneumoniaDocumento21 páginasBroncho PneumoniaRiad GagahAinda não há avaliações
- Metod Terapiya Lechebnoe Delo Fakul'tet Inostranyx Studentov-006Documento29 páginasMetod Terapiya Lechebnoe Delo Fakul'tet Inostranyx Studentov-006Nishani SatiyaseelanAinda não há avaliações
- Lung AbcessDocumento11 páginasLung AbcessGul SapiAinda não há avaliações
- Sputum Exam GuideDocumento36 páginasSputum Exam GuideSari Bunga Mastina0% (1)
- Bronchial Asthma ThesisDocumento33 páginasBronchial Asthma ThesisAbdul Hafiz40% (5)
- Histological Features of Rats' Normal Lung Tissue: Dr. Koptyev M.MDocumento6 páginasHistological Features of Rats' Normal Lung Tissue: Dr. Koptyev M.MManMan AR-llAinda não há avaliações
- Nursing Care Management - 112Documento67 páginasNursing Care Management - 112Ong KarlAinda não há avaliações
- CompilationDocumento24 páginasCompilationKath RubioAinda não há avaliações
- Understanding Bronchiectasis: Causes, Symptoms and TreatmentDocumento60 páginasUnderstanding Bronchiectasis: Causes, Symptoms and TreatmentArulAinda não há avaliações
- PneumoniaDocumento14 páginasPneumoniaDrashti Dewani100% (1)
- SGL6 - CoughDocumento63 páginasSGL6 - CoughDarawan MirzaAinda não há avaliações
- Bronchiectasis OkDocumento60 páginasBronchiectasis OkImmanuelAinda não há avaliações
- Week 1 NotesDocumento61 páginasWeek 1 NotesKhan BuzAinda não há avaliações
- 6.lung AbscessDocumento13 páginas6.lung AbscessManushi HenadeeraAinda não há avaliações
- Respiration CH 43.Dr SarahDocumento59 páginasRespiration CH 43.Dr Sarahaiman siddiquiAinda não há avaliações
- Matthew E. Levison: PneumoniaDocumento30 páginasMatthew E. Levison: PneumoniaWira AisyaAinda não há avaliações
- Assignment NO 1: Name:Adeel Afzal Section: C Sap I'd: 70126263 Assignment: Physiology Submitted To: DR Urfah ZaighamDocumento6 páginasAssignment NO 1: Name:Adeel Afzal Section: C Sap I'd: 70126263 Assignment: Physiology Submitted To: DR Urfah ZaighamAdeel AfzalAinda não há avaliações
- Lesson25 (2) - Management of Chronic CoughDocumento27 páginasLesson25 (2) - Management of Chronic CoughAditi JainAinda não há avaliações
- Pathology of The Respiratory System 2Documento76 páginasPathology of The Respiratory System 2Fabian ChapimaAinda não há avaliações
- Respiratory SystemDocumento43 páginasRespiratory SystemMaxxdlc 16Ainda não há avaliações
- Approach To Interstitial Lung Disease 1Documento33 páginasApproach To Interstitial Lung Disease 1MichaelAinda não há avaliações
- PBL Copd: 1) Mechanics of RespirationDocumento34 páginasPBL Copd: 1) Mechanics of RespirationAhmadAinda não há avaliações
- How to Collect Sputum SamplesDocumento14 páginasHow to Collect Sputum SamplesAira AlaroAinda não há avaliações
- Respiratory Bronchioles, Alveolar Ducts, and Alveoli ExplainedDocumento70 páginasRespiratory Bronchioles, Alveolar Ducts, and Alveoli ExplainedtazeAinda não há avaliações
- Respiratory diseases guideDocumento71 páginasRespiratory diseases guideZafir SharifAinda não há avaliações
- Asthma: EpidemiologyDocumento4 páginasAsthma: EpidemiologyJerome PrattAinda não há avaliações
- Diseases of Respiratory SystemDocumento23 páginasDiseases of Respiratory SystemMarchelle Fae EsmallaAinda não há avaliações
- Asthma: Pre by Lect. ZAHID REHMAN Ipms (Kmu)Documento29 páginasAsthma: Pre by Lect. ZAHID REHMAN Ipms (Kmu)SHAFI ULLAHAinda não há avaliações
- Cystic FibrosisDocumento13 páginasCystic Fibrosisgandhialpit100% (4)
- Thorax00193 0009 PDFDocumento10 páginasThorax00193 0009 PDFhotmart ventasAinda não há avaliações
- Jordan A. Mamalumpong Bsn-3 Clinical Instructor: Ma. Antonietta Edris Assignments For NCM 112 A. GlossaryDocumento11 páginasJordan A. Mamalumpong Bsn-3 Clinical Instructor: Ma. Antonietta Edris Assignments For NCM 112 A. GlossaryJordan Abosama MamalumpongAinda não há avaliações
- Lung Disease PicsDocumento169 páginasLung Disease PicsDr-Mohammad Ali-Fayiz Al TamimiAinda não há avaliações
- Cyto Lungtumorbook1Documento104 páginasCyto Lungtumorbook1ixAinda não há avaliações
- Respiratory DisordersDocumento20 páginasRespiratory DisordersjeromeAinda não há avaliações
- Broncho PneumoniaDocumento23 páginasBroncho Pneumoniaanon-84769398% (43)
- Part 1 & 2 - Pulmonary Disease & Non-Neoplastic Lung PathologyDocumento89 páginasPart 1 & 2 - Pulmonary Disease & Non-Neoplastic Lung PathologyJeanPaule JoumaaAinda não há avaliações
- Acute Lung Abscesses. Definition of The Idea. Classification. Etiology and Pathogenesis. Clinical Picture. Diagnosis.Documento6 páginasAcute Lung Abscesses. Definition of The Idea. Classification. Etiology and Pathogenesis. Clinical Picture. Diagnosis.Lucas Victor AlmeidaAinda não há avaliações
- COPD AND ASTHMA LAB REPORTDocumento6 páginasCOPD AND ASTHMA LAB REPORTIlhaashini krishnanAinda não há avaliações
- COPD & RLDDocumento17 páginasCOPD & RLDhis.thunder122Ainda não há avaliações
- Chapter 27Documento6 páginasChapter 27monster40lbsAinda não há avaliações
- The Kursk State Medical University: Lecture For Self-Training of 6-th Medical Course English-Speaking StudentsDocumento15 páginasThe Kursk State Medical University: Lecture For Self-Training of 6-th Medical Course English-Speaking StudentsDaniel FunkAinda não há avaliações
- Medical Mnemonic Sketches : Pulmonary DiseasesNo EverandMedical Mnemonic Sketches : Pulmonary DiseasesAinda não há avaliações
- Pulmonary Endocrine Pathology: Endocrine Cells and Endocrine Tumours of the LungNo EverandPulmonary Endocrine Pathology: Endocrine Cells and Endocrine Tumours of the LungAinda não há avaliações
- Causes and Possible Prevention of Asthma and AllergiesNo EverandCauses and Possible Prevention of Asthma and AllergiesAinda não há avaliações
- Prof. Koch's Method to Cure Tuberculosis Popularly TreatedNo EverandProf. Koch's Method to Cure Tuberculosis Popularly TreatedAinda não há avaliações
- MICRO 8th & 9th LEDocumento1 páginaMICRO 8th & 9th LEchocoholic potchiAinda não há avaliações
- Justine's Group Integrated MethodDocumento9 páginasJustine's Group Integrated Methodchocoholic potchiAinda não há avaliações
- Birth History-Feeding PediaDocumento2 páginasBirth History-Feeding Pediachocoholic potchiAinda não há avaliações
- LMMJ - Midterms 1.1 - Medico-Legal Aspects of Physical Injuries I TransDocumento6 páginasLMMJ - Midterms 1.1 - Medico-Legal Aspects of Physical Injuries I Transchocoholic potchiAinda não há avaliações
- TeachingstratDocumento21 páginasTeachingstratchocoholic potchiAinda não há avaliações
- Bio DataDocumento1 páginaBio Datachocoholic potchiAinda não há avaliações
- 2b 2c Fifi ClostridiumDocumento7 páginas2b 2c Fifi Clostridiumchocoholic potchi100% (1)
- Pathogenesis of Atherosclerosis: These Are The Composition of YourDocumento4 páginasPathogenesis of Atherosclerosis: These Are The Composition of Yourchocoholic potchiAinda não há avaliações
- Pathogenesis of Atherosclerosis: These Are The Composition of YourDocumento4 páginasPathogenesis of Atherosclerosis: These Are The Composition of Yourchocoholic potchiAinda não há avaliações
- Bio DataDocumento1 páginaBio Datachocoholic potchiAinda não há avaliações
- Pre RegisformDocumento1 páginaPre Regisformchocoholic potchiAinda não há avaliações
- Activity Based Teaching Strategies: Advantages and DisadvantagesDocumento4 páginasActivity Based Teaching Strategies: Advantages and Disadvantageschocoholic potchiAinda não há avaliações
- Cardiac Cath LabDocumento4 páginasCardiac Cath Labchocoholic potchiAinda não há avaliações
- Personality SketchDocumento1 páginaPersonality Sketchchocoholic potchiAinda não há avaliações
- Bio DataDocumento1 páginaBio Datachocoholic potchiAinda não há avaliações
- Traditional Teaching Strategies: Group 1Documento34 páginasTraditional Teaching Strategies: Group 1chocoholic potchiAinda não há avaliações
- Activity-Based Teaching Strategy: Group 3Documento26 páginasActivity-Based Teaching Strategy: Group 3chocoholic potchiAinda não há avaliações
- I. Computer Technology and Learning: Role of The StudentDocumento6 páginasI. Computer Technology and Learning: Role of The Studentchocoholic potchiAinda não há avaliações
- FWR Teaching MethodsDocumento6 páginasFWR Teaching Methodschocoholic potchiAinda não há avaliações
- Integrated Method (FWR)Documento3 páginasIntegrated Method (FWR)chocoholic potchi100% (4)
- Final Written Report Teaching StratDocumento8 páginasFinal Written Report Teaching Stratchocoholic potchiAinda não há avaliações
- Adhesives, Staining, MountingDocumento10 páginasAdhesives, Staining, Mountingchocoholic potchiAinda não há avaliações
- Learning PrinciplesDocumento20 páginasLearning Principleschocoholic potchiAinda não há avaliações
- Tissue Sectioning & CuttingDocumento50 páginasTissue Sectioning & Cuttingchocoholic potchiAinda não há avaliações
- Hemodynamic Disorders: Ma. Minda Luz M. Manuguid, M.DDocumento59 páginasHemodynamic Disorders: Ma. Minda Luz M. Manuguid, M.Dchocoholic potchiAinda não há avaliações
- CC 3Documento19 páginasCC 3chocoholic potchiAinda não há avaliações
- Gen Path IntroDocumento36 páginasGen Path Introchocoholic potchiAinda não há avaliações
- Group 9 Pleural Fluid A 36-YearDocumento6 páginasGroup 9 Pleural Fluid A 36-Yearchocoholic potchiAinda não há avaliações
- Tension Pneumothorax: Modifiable FactorsDocumento3 páginasTension Pneumothorax: Modifiable FactorsJustin MaverickAinda não há avaliações
- Pae - Respiratory SystemDocumento11 páginasPae - Respiratory SystemMegha ProjectsAinda não há avaliações
- Science Test: Chapter I Respiratory and Circulatory System Term I, Semester IDocumento4 páginasScience Test: Chapter I Respiratory and Circulatory System Term I, Semester IimandaAinda não há avaliações
- Chronic Obstructive Pulmonary Disease COPDDocumento2 páginasChronic Obstructive Pulmonary Disease COPDJoseph Angelo OcampoAinda não há avaliações
- Respiratory System: Study: Pulmonology Physician: Pulmonologist Function: Exchange of GasesDocumento5 páginasRespiratory System: Study: Pulmonology Physician: Pulmonologist Function: Exchange of GasesSakshi BishnoiAinda não há avaliações
- Science 6 Living Things and Their Environment Earth and Space As Reviewed by SME 1Documento36 páginasScience 6 Living Things and Their Environment Earth and Space As Reviewed by SME 1Elma Ortega CamionAinda não há avaliações
- Airway Obstruction Post COVID CaseDocumento48 páginasAirway Obstruction Post COVID CaseCindy GoAinda não há avaliações
- Lower Respiratory Disorders Part 1Documento70 páginasLower Respiratory Disorders Part 1Joseph Krafft100% (1)
- B4 TH NXT Song ANALYSISDocumento23 páginasB4 TH NXT Song ANALYSISAlisah Magaya100% (1)
- Neet - Combined Test - 2 (P, C, B) - 06.08.2017Documento20 páginasNeet - Combined Test - 2 (P, C, B) - 06.08.2017Sankar KumarasamyAinda não há avaliações
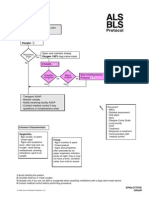
- Epiglottitis Croup ALS BLSDocumento1 páginaEpiglottitis Croup ALS BLStamara4668Ainda não há avaliações
- Grade 9 Chapter 1 Revision Worksheet - 1Documento3 páginasGrade 9 Chapter 1 Revision Worksheet - 1Abdullah AkmalAinda não há avaliações
- Referat HemothoraksDocumento28 páginasReferat HemothoraksitsmediAinda não há avaliações
- CBSE Class 7 Science MCQs-Respiration in OrganismsDocumento2 páginasCBSE Class 7 Science MCQs-Respiration in Organismssiba padhy100% (3)
- Nitrous Oxide in Emergency MedicineDocumento4 páginasNitrous Oxide in Emergency MedicinenumaidecatAinda não há avaliações
- BTS Clinical Statement On Air TravelDocumento22 páginasBTS Clinical Statement On Air TravelAli SemajAinda não há avaliações
- Resource Unit in OxygenationDocumento24 páginasResource Unit in OxygenationlouradelAinda não há avaliações
- Fiche de Sécurité TEF GELDocumento3 páginasFiche de Sécurité TEF GELNur IslamiaAinda não há avaliações
- Ventilator ABV-A Service ManualDocumento23 páginasVentilator ABV-A Service Manualbashaar ahmedAinda não há avaliações
- Respiratory Assessment FindingsDocumento197 páginasRespiratory Assessment Findingsannatw100% (2)
- Pathology Lecture 1 MSADocumento6 páginasPathology Lecture 1 MSAcejix87209Ainda não há avaliações
- Articulo Asma Felina 1 PDFDocumento5 páginasArticulo Asma Felina 1 PDFTania GonzalezAinda não há avaliações
- Vet. Internal Medicine Text BookDocumento674 páginasVet. Internal Medicine Text Bookuhgl hgluvtm100% (5)
- ASPEN Nutrition Support During Prone PositionDocumento5 páginasASPEN Nutrition Support During Prone PositionAlimah YasminAinda não há avaliações
- Bronchiectasis Pa Tho Physiology, Presentation and ManagementDocumento8 páginasBronchiectasis Pa Tho Physiology, Presentation and ManagementCristhian MellaAinda não há avaliações
- Chest PBLDocumento2 páginasChest PBLRamish IrfanAinda não há avaliações
- BSC Nursing SyllDocumento218 páginasBSC Nursing SyllKiran KhasaAinda não há avaliações
- Oriental Breathing Terapy NakamuraDocumento146 páginasOriental Breathing Terapy Nakamurahcorzo100% (2)