Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- ACLS 2020 Algorithms: American Heart Association 2020 GuidelinesDocumento8 páginasACLS 2020 Algorithms: American Heart Association 2020 GuidelinesNofi Nurina100% (4)
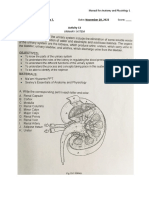
- Urinary SystemDocumento5 páginasUrinary SystemJushelle Anne Tigoy Pilare100% (1)
- Physicians ListingDocumento46 páginasPhysicians ListingMahesh SeelamAinda não há avaliações
- Ophtha Imp MCQ FmgeDocumento54 páginasOphtha Imp MCQ Fmgevikas prajapatAinda não há avaliações
- Essential Intrapartum Care UpdatedDocumento11 páginasEssential Intrapartum Care UpdatedRica PeñanoAinda não há avaliações
- Policies and Procedures For Ambulance ServiceDocumento3 páginasPolicies and Procedures For Ambulance ServiceLymberth Benalla100% (1)
- Nursing ICUDocumento2 páginasNursing ICUKomal Tomar50% (2)
- RENAP 2009 Training SchedulesDocumento3 páginasRENAP 2009 Training SchedulesNoel100% (4)
- Produk e Katalog 2023Documento12 páginasProduk e Katalog 2023Bedo Sari AntonAinda não há avaliações
- Andersson 2003Documento6 páginasAndersson 2003IngrydCamposAinda não há avaliações
- BSS 2018Documento24 páginasBSS 2018gumoha01Ainda não há avaliações
- CystosDocumento1 páginaCystosgeorgeloto12Ainda não há avaliações
- 1.2 Daftar Kode Diagnosa Dan TindakanDocumento45 páginas1.2 Daftar Kode Diagnosa Dan Tindakaneva adityaAinda não há avaliações
- Talbot DeclDocumento5 páginasTalbot DeclCassandra FairbanksAinda não há avaliações
- Guidance For Safer HandlingDocumento36 páginasGuidance For Safer HandlingFlorentina GasttiAinda não há avaliações
- GENESIS II Surgical Technique DCFDocumento46 páginasGENESIS II Surgical Technique DCFMazilo VictorAinda não há avaliações
- Dexamethasone For Postoperative Nausea and Vomiting in Papillary Thyroid Carcinoma PatientsA Randomized Clinical TrialDocumento14 páginasDexamethasone For Postoperative Nausea and Vomiting in Papillary Thyroid Carcinoma PatientsA Randomized Clinical Trialguohong huAinda não há avaliações
- 03 In-Office Endoscopic Laryngeal Laser ProceduresDocumento7 páginas03 In-Office Endoscopic Laryngeal Laser ProceduresG WAinda não há avaliações
- Ebstein Anomaly in The Adult PatientDocumento11 páginasEbstein Anomaly in The Adult PatientRJMAinda não há avaliações
- WFA Competency LevelsDocumento5 páginasWFA Competency LevelsTroy Lyons DunowAinda não há avaliações
- HerniasDocumento64 páginasHerniasKalpana SubediAinda não há avaliações
- Orion Prototype Final WalkthroughDocumento16 páginasOrion Prototype Final Walkthroughcsedwards03Ainda não há avaliações
- ECG WorksheetDocumento4 páginasECG WorksheetNikki GuisonAinda não há avaliações
- Salam Saleh DaradkehDocumento4 páginasSalam Saleh DaradkehRuli OktariveriusAinda não há avaliações
- Hollis V Dow Corning CorporationDocumento2 páginasHollis V Dow Corning CorporationAlice Jiang100% (1)
- AIIMS NORCET 2022 Memory Based Paper 11th September 2022 EnglishDocumento20 páginasAIIMS NORCET 2022 Memory Based Paper 11th September 2022 EnglishMata BharatAinda não há avaliações
- Benign Prostatic HyperplasiaDocumento9 páginasBenign Prostatic Hyperplasiaanju rachel joseAinda não há avaliações
- Evaluation and Management of Right-Sided Heart FailureDocumento45 páginasEvaluation and Management of Right-Sided Heart FailureFreddy PanjaitanAinda não há avaliações
- Final Ugib Sec To BpudDocumento17 páginasFinal Ugib Sec To BpudBaby Kate BONGCARASAinda não há avaliações
- Assessment of Right Ventricular FunctionDocumento41 páginasAssessment of Right Ventricular FunctionAditya MadhavpeddiAinda não há avaliações