Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Ujian KV KoasDocumento2 páginasUjian KV KoasPratama Aditya BiantoroAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- METAFISIKADocumento11 páginasMETAFISIKAPratama Aditya BiantoroAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Baris OtluDocumento6 páginasBaris OtluPratama Aditya BiantoroAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Happy Birthday SongDocumento1 páginaHappy Birthday SongPratama Aditya BiantoroAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Blank DocumentDocumento1 páginaBlank DocumentPratama Aditya BiantoroAinda não há avaliações
- Algo Tachycardia PDFDocumento1 páginaAlgo Tachycardia PDFYudhistira AdiAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- BMJ 335 7630 CR 01147 Vaginal DischargeDocumento5 páginasBMJ 335 7630 CR 01147 Vaginal DischargeHassan Abdullah AL-balushiAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Immunological Parameters Associated With Vitiligo Treatments - A Literature Review Based On Clinical StudiesDocumento5 páginasImmunological Parameters Associated With Vitiligo Treatments - A Literature Review Based On Clinical StudiesPratama Aditya BiantoroAinda não há avaliações
- Daftar PustakaDocumento1 páginaDaftar PustakaPratama Aditya BiantoroAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Logo Fkuy Yng BenarDocumento1 páginaLogo Fkuy Yng BenarPutri MaulinaAinda não há avaliações
- Specific Immunotherapy in Atopic DermatitisDocumento9 páginasSpecific Immunotherapy in Atopic DermatitisPratama Aditya BiantoroAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Practice Essentials: Essential Update: New Guidelines From KDIGODocumento13 páginasPractice Essentials: Essential Update: New Guidelines From KDIGOPratama Aditya BiantoroAinda não há avaliações
- Neurological Examination 1200430093249063 3Documento33 páginasNeurological Examination 1200430093249063 3Pratama Aditya BiantoroAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Selection of Proper Antiepileptic Drugs: 1 IntroductionDocumento1 páginaSelection of Proper Antiepileptic Drugs: 1 IntroductionPratama Aditya BiantoroAinda não há avaliações
- Ceo 6 90Documento4 páginasCeo 6 90Pratama Aditya BiantoroAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- 2012 JOSPT Guidelines LowBackPainDocumento58 páginas2012 JOSPT Guidelines LowBackPain1RogerioAinda não há avaliações
- WJG 19 7247Documento12 páginasWJG 19 7247Pratama Aditya BiantoroAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- AIUM Practice GuidelineDocumento12 páginasAIUM Practice Guidelineg1381821Ainda não há avaliações
- Multidisciplinary Approach in Advanced Cancer of The Oral Cavity: Outcome With Neoadjuvant Chemotherapy According To Intention-to-Treat Local TherapyDocumento10 páginasMultidisciplinary Approach in Advanced Cancer of The Oral Cavity: Outcome With Neoadjuvant Chemotherapy According To Intention-to-Treat Local TherapyPratama Aditya BiantoroAinda não há avaliações
- Cocaine Use and StrokeDocumento7 páginasCocaine Use and StrokePratama Aditya BiantoroAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- DLL - Mapeh 3 - Q1 - W9Documento2 páginasDLL - Mapeh 3 - Q1 - W9Rucelle Mae Fernandez ArbolerasAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- MUNGGODocumento17 páginasMUNGGOJenny Joy B. Fortin100% (2)
- Food CombiningDocumento2 páginasFood Combiningmagda___Ainda não há avaliações
- Jalgaon IIDocumento9 páginasJalgaon IIRam K YadavAinda não há avaliações
- 4ds0315e P2 (F)Documento1 página4ds0315e P2 (F)nagravAinda não há avaliações
- Enzyme PPT 12 PDFDocumento42 páginasEnzyme PPT 12 PDFAnonymous wY9ogndU100% (1)
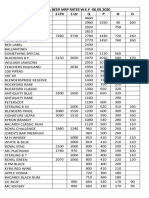
- Liquor & Beer MRP Rates Wef 17.12.2019 (1) - 1Documento2 páginasLiquor & Beer MRP Rates Wef 17.12.2019 (1) - 1Kondu Krishna Vamsi ChowdaryAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Aа reading drillDocumento2 páginasAа reading drillДіана МатковаAinda não há avaliações
- Suga-Lik® - Dairy SupplementsDocumento2 páginasSuga-Lik® - Dairy SupplementsHemlata LodhaAinda não há avaliações
- Phrasal Verbs - Make and DoDocumento6 páginasPhrasal Verbs - Make and DoCarolina AndreaAinda não há avaliações
- Research Report VitagenDocumento11 páginasResearch Report Vitagenaina sofiaAinda não há avaliações
- Resources DistributionDocumento10 páginasResources DistributionDarshan KanganeAinda não há avaliações
- Easy Exercises On Reported SpeechDocumento4 páginasEasy Exercises On Reported SpeechminhanhAinda não há avaliações
- Lteif Anthony E02e - PlantsDocumento2 páginasLteif Anthony E02e - PlantsSaiid GhimrawiAinda não há avaliações
- Parish Pump July 2013Documento44 páginasParish Pump July 2013Debden.orgAinda não há avaliações
- Pippa and Pop Pippa and Pop Teacher Book 1 U5 9781108928298 Sample ContentDocumento27 páginasPippa and Pop Pippa and Pop Teacher Book 1 U5 9781108928298 Sample ContentMelissa ParedesAinda não há avaliações
- Photo 1: Typical Unprotected and Eroding SlopeDocumento7 páginasPhoto 1: Typical Unprotected and Eroding SlopeMarshall BravestarAinda não há avaliações
- 10englishb Grammar Test 1 2008Documento3 páginas10englishb Grammar Test 1 2008Anonymous rePT5rCrAinda não há avaliações
- TS24 (EC) V01en Plant ProductionDocumento12 páginasTS24 (EC) V01en Plant ProductionlabuniciAinda não há avaliações
- Perten Falling Number FN SeriesDocumento28 páginasPerten Falling Number FN SeriesOSMANAinda não há avaliações
- The Punjab Pure Food Rules 2007Documento242 páginasThe Punjab Pure Food Rules 2007Waris Arslan0% (1)
- Polyethylene HDPE XS 10 B: Content: - Technical Data Sheet - Regulatory CertificateDocumento9 páginasPolyethylene HDPE XS 10 B: Content: - Technical Data Sheet - Regulatory CertificateoscarpetroflexAinda não há avaliações
- Croatia 5 KvarnerDocumento37 páginasCroatia 5 KvarnermumikaAinda não há avaliações
- Acceptability and Use of Cereal-Based Foods in Refugee Camps: Case-Studies From Nepal, Ethiopia, and TanzaniaDocumento137 páginasAcceptability and Use of Cereal-Based Foods in Refugee Camps: Case-Studies From Nepal, Ethiopia, and TanzaniaOxfamAinda não há avaliações
- Science Section A UPSRDocumento2 páginasScience Section A UPSRvinno8556% (9)
- Africa-Europe Cook BookDocumento62 páginasAfrica-Europe Cook BookAmy SAinda não há avaliações
- A Case Study On KFCDocumento18 páginasA Case Study On KFCManish Singh89% (18)
- Bryan Babylon Café/Naya International LLCDocumento2 páginasBryan Babylon Café/Naya International LLCKBTXAinda não há avaliações
- A Modest ProposalDocumento12 páginasA Modest ProposalcarlosliraAinda não há avaliações
- Unleashing The Flavorful Journey - Exploring The Success Story of MTR FoodsDocumento11 páginasUnleashing The Flavorful Journey - Exploring The Success Story of MTR FoodsPrabha DineshAinda não há avaliações
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)No EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Nota: 4 de 5 estrelas4/5 (378)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyNo EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyNota: 4.5 de 5 estrelas4.5/5 (2)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNo EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeAinda não há avaliações
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonNo EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonNota: 3.5 de 5 estrelas3.5/5 (33)