Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Strength and Conditioning Coach or Sports Performance Coach or FDocumento3 páginasStrength and Conditioning Coach or Sports Performance Coach or Fapi-121340325Ainda não há avaliações
- Lecture 9 Reading Assignment 2Documento9 páginasLecture 9 Reading Assignment 2Dennis KorirAinda não há avaliações
- Engineering A Healthy Body: Career CatalystDocumento6 páginasEngineering A Healthy Body: Career CatalystB6D4N0Ainda não há avaliações
- Millennial Preferences Toward Treating Minor DiseasesDocumento47 páginasMillennial Preferences Toward Treating Minor DiseasesMa Angelica Edison SesucaAinda não há avaliações
- The Role of A Pastor As A CounselorDocumento5 páginasThe Role of A Pastor As A Counselorkhetsiwe gule100% (2)
- Psychological AdjustmentDocumento100 páginasPsychological AdjustmentRagil Adist Surya PutraAinda não há avaliações
- ICD 10overviewDocumento4 páginasICD 10overviewObat Dot In100% (1)
- What Is Primary ComplexDocumento18 páginasWhat Is Primary ComplexMary Cruz100% (6)
- Drug-Induced Liver Disease.Documento16 páginasDrug-Induced Liver Disease.Dr. Ammar Khalil100% (1)
- LEEDEN Basic 사용재료 - 23-10-30Documento28 páginasLEEDEN Basic 사용재료 - 23-10-30이상민Ainda não há avaliações
- CANINE-Medical Management of Chronic Otitis in DogsDocumento11 páginasCANINE-Medical Management of Chronic Otitis in Dogstaner_soysuren100% (1)
- Antigens Antibodies and VaccinesDocumento4 páginasAntigens Antibodies and Vaccinesapi-299996815Ainda não há avaliações
- MycetomaDocumento26 páginasMycetomaTummalapalli Venkateswara RaoAinda não há avaliações
- English For Medical Students CoursebookDocumento117 páginasEnglish For Medical Students CoursebookNevfel100% (10)
- Burnout - Existential Meaning and Possibilities of Prevention (Alfried Längle)Documento16 páginasBurnout - Existential Meaning and Possibilities of Prevention (Alfried Längle)abaeram2Ainda não há avaliações
- Soyabean Milk ReportDocumento10 páginasSoyabean Milk Reportprakhalgoyal100% (1)
- Necrotic Enteritis in ChickensDocumento3 páginasNecrotic Enteritis in ChickensHendra PranotogomoAinda não há avaliações
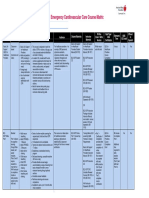
- Emergency Cardiovascular Care Course MatrixDocumento15 páginasEmergency Cardiovascular Care Course MatrixJesus M. Espinosa EchavarriaAinda não há avaliações
- TuberculosisDocumento16 páginasTuberculosisjojolim18100% (1)
- Morning Report 2Documento16 páginasMorning Report 2erniAinda não há avaliações
- Adulthood & Geriatric PsychiatryDocumento13 páginasAdulthood & Geriatric PsychiatryPernel Jose Alam MicuboAinda não há avaliações
- ReflexologyDocumento27 páginasReflexologyJessica Jones100% (1)
- Revised Sample Scheme of Work and Lesson Plan For Nursing Class (Koya)Documento6 páginasRevised Sample Scheme of Work and Lesson Plan For Nursing Class (Koya)NATHANIEL YERIAinda não há avaliações
- Devarajan, Dss DGN ArdsDocumento4 páginasDevarajan, Dss DGN ArdsrantiadrianiAinda não há avaliações
- CPG Abnormal Labor and Delivery PDFDocumento29 páginasCPG Abnormal Labor and Delivery PDFKarl Jimenez Separa100% (2)
- Crystalls & Mineralls MeaningsDocumento26 páginasCrystalls & Mineralls MeaningsCandice Cogburn100% (1)
- Assessing Nutrition in Patients With Chronic Kidney Disease by Kimberly Thompson, MS, RD, LDNDocumento23 páginasAssessing Nutrition in Patients With Chronic Kidney Disease by Kimberly Thompson, MS, RD, LDNCarlos RaiolAinda não há avaliações
- Painful Intramuscular Lipoma of The Infraspinatus Unusual Location and PresentationDocumento4 páginasPainful Intramuscular Lipoma of The Infraspinatus Unusual Location and PresentationWewik PenaAinda não há avaliações
- Comprehensive Assessment Diagnosis and Treatment Planning of Severe Periodontal DiseaseDocumento9 páginasComprehensive Assessment Diagnosis and Treatment Planning of Severe Periodontal DiseaseJOHAYMEN MANGORSIAinda não há avaliações
- Running Head: Client Teaching Wound Care 1Documento3 páginasRunning Head: Client Teaching Wound Care 1Jerome Lazaro LumanogAinda não há avaliações