Você também pode gostar
- Colecistogastrostomia-Biopsia de HigadoDocumento8 páginasColecistogastrostomia-Biopsia de HigadoWildor Herrera GuevaraAinda não há avaliações
- ZollingerDocumento5 páginasZollingerSantiago Xicotencatl MendezAinda não há avaliações
- Urinary Diversion Following Cystectomy: EAU Update SeriesDocumento9 páginasUrinary Diversion Following Cystectomy: EAU Update SeriesmoetazAinda não há avaliações
- Colectomia Total PDFDocumento11 páginasColectomia Total PDFWildor Herrera GuevaraAinda não há avaliações
- Been Abandoned in Favor of Hetero-/ortho-Topic Pouches.: Heterotopic Continent DiversionDocumento1 páginaBeen Abandoned in Favor of Hetero-/ortho-Topic Pouches.: Heterotopic Continent DiversioncesaliapAinda não há avaliações
- Total Pelvic ExenterationDocumento13 páginasTotal Pelvic ExenterationRirin Wahyuni100% (1)
- Colonic Interposition For Benign DiseaseDocumento18 páginasColonic Interposition For Benign DiseaseOhana S.Ainda não há avaliações
- Los Terrybles Book TeamDocumento6 páginasLos Terrybles Book TeamWildor Herrera GuevaraAinda não há avaliações
- Los Terrybles Book TeamDocumento10 páginasLos Terrybles Book TeamWildor Herrera GuevaraAinda não há avaliações
- Colectomia Izquierda, Anastomosis Termino-TerminalDocumento11 páginasColectomia Izquierda, Anastomosis Termino-TerminalWildor Herrera GuevaraAinda não há avaliações
- Biliary Enteric BypassDocumento25 páginasBiliary Enteric BypassAlexandru Ferdohleb100% (1)
- Abdominoperineal Resection MilesDocumento17 páginasAbdominoperineal Resection MilesHugoAinda não há avaliações
- Chapter 20Documento14 páginasChapter 20Syafithria WuAinda não há avaliações
- Oesophagocoloplasty For Corrosive Oesophageal Stricture: AbstractDocumento12 páginasOesophagocoloplasty For Corrosive Oesophageal Stricture: AbstractSpandan KadamAinda não há avaliações
- Mainz II Surgery IllustratedDocumento25 páginasMainz II Surgery IllustratedPurvi ParikhAinda não há avaliações
- Urinary DiversionDocumento44 páginasUrinary Diversionminnalesri100% (1)
- Sleeve-Gastrectomy 2011 BrethauerDocumento15 páginasSleeve-Gastrectomy 2011 BrethauerDavid Schnettler RodriguezAinda não há avaliações
- Colostomy & Colostomy CareDocumento56 páginasColostomy & Colostomy Careapi-3722454100% (31)
- CHOLECYSTECTOMYDocumento6 páginasCHOLECYSTECTOMYJagannath DasAinda não há avaliações
- Img 0076Documento1 páginaImg 0076O'jays NavarroAinda não há avaliações
- CholecystectomyDocumento9 páginasCholecystectomyAmyandAinda não há avaliações
- Los Terrybles Book TeamDocumento6 páginasLos Terrybles Book TeamWildor Herrera GuevaraAinda não há avaliações
- Colecist Anterograd DeschisDocumento5 páginasColecist Anterograd DeschisAna MariaAinda não há avaliações
- Uretrostomia AtlasDocumento10 páginasUretrostomia AtlasquirinalAinda não há avaliações
- ColostomyDocumento45 páginasColostomydrqiekiAinda não há avaliações
- Diagnosis & ManagementDocumento36 páginasDiagnosis & ManagementKenMAinda não há avaliações
- Suprapubic CatheterizationDocumento34 páginasSuprapubic CatheterizationalfiAinda não há avaliações
- Rectovaginal Fistula RepairDocumento3 páginasRectovaginal Fistula Repairnaftalina7Ainda não há avaliações
- ColostomyDocumento60 páginasColostomymathisyncAinda não há avaliações
- Pi Is 2213576614000049Documento3 páginasPi Is 2213576614000049Ditha FadhilaAinda não há avaliações
- Case ReportDocumento5 páginasCase ReportAmmar magdyAinda não há avaliações
- Appendicectomy Step by Step PDFDocumento9 páginasAppendicectomy Step by Step PDFOlugbenga A Adetunji100% (1)
- Hepatico JDocumento4 páginasHepatico Jcharie2Ainda não há avaliações
- Dismembered PyeloplastyDocumento7 páginasDismembered PyeloplastymichaelAinda não há avaliações
- ColectomyDocumento9 páginasColectomyAgung Choro de ObesAinda não há avaliações
- Cholelith MGT - 2Documento33 páginasCholelith MGT - 2KenMAinda não há avaliações
- Equine Abdominal SurgeryDocumento76 páginasEquine Abdominal SurgeryasheneyAinda não há avaliações
- Dimatingcal, Warda M. BSN14D Group 24 (Laparoscopic Feeding Jejunostomy)Documento18 páginasDimatingcal, Warda M. BSN14D Group 24 (Laparoscopic Feeding Jejunostomy)WARDA DIMATINGCALAinda não há avaliações
- By Abayneh Ayele (Ieso Student) Wollo UniversityDocumento68 páginasBy Abayneh Ayele (Ieso Student) Wollo UniversitydenekeAinda não há avaliações
- Pancreaticogastrostomy: Gerard V. Aranha, MD, FRCSC, FACSDocumento7 páginasPancreaticogastrostomy: Gerard V. Aranha, MD, FRCSC, FACSBogdan TrandafirAinda não há avaliações
- Cholecystectomy: Cholecystectomy (Pronounced / Kɒləsɪs Tɛktəmi/, Plural: Cholecystectomies) Is TheDocumento3 páginasCholecystectomy: Cholecystectomy (Pronounced / Kɒləsɪs Tɛktəmi/, Plural: Cholecystectomies) Is Thejosias_jorgio1Ainda não há avaliações
- Cholecystectomy (: Laparoscopic GallstonesDocumento4 páginasCholecystectomy (: Laparoscopic GallstonesAlexia BatungbacalAinda não há avaliações
- Laparoscopic Cholecystectomy - StatPearls - NCBI BookshelfDocumento1 páginaLaparoscopic Cholecystectomy - StatPearls - NCBI BookshelfOmar HamwiAinda não há avaliações
- Cholecystectomy: Navigation SearchDocumento4 páginasCholecystectomy: Navigation SearchMohammed OmerAinda não há avaliações
- IleostomyDocumento3 páginasIleostomysgod34Ainda não há avaliações
- Open Cholecystectomy ReportDocumento7 páginasOpen Cholecystectomy ReportjosephcloudAinda não há avaliações
- Esophagectomy: Right Thoracotomy and Laparotomy With Cervical AnastomosisDocumento7 páginasEsophagectomy: Right Thoracotomy and Laparotomy With Cervical AnastomosissunnyAinda não há avaliações
- Remove Them Within A Week. Mainz Neobladder: Chapter 189: Supravesical Urinary DiversionDocumento1 páginaRemove Them Within A Week. Mainz Neobladder: Chapter 189: Supravesical Urinary DiversioncesaliapAinda não há avaliações
- Part 7 Pyeloroplasty: Quick and BloodlessDocumento31 páginasPart 7 Pyeloroplasty: Quick and BloodlessAnonymous MmiBnqnDyAinda não há avaliações
- Liver Transplantation For Biliary Atresia : Thomas E. Starz), M.D., Ph.D. Carlos O. Esquivel, M.D., PH.DDocumento8 páginasLiver Transplantation For Biliary Atresia : Thomas E. Starz), M.D., Ph.D. Carlos O. Esquivel, M.D., PH.DPratita Jati PermatasariAinda não há avaliações
- Cierre de ColostomiaDocumento9 páginasCierre de ColostomiaWildor Herrera GuevaraAinda não há avaliações
- Articulo 1 Quiste ColeDocumento4 páginasArticulo 1 Quiste ColeMaria Elena VinuezaAinda não há avaliações
- Surgical Management of Biliary Diseases Jamie R. Bellah, DVM, Diplomate ACVSDocumento2 páginasSurgical Management of Biliary Diseases Jamie R. Bellah, DVM, Diplomate ACVSArokiya Anand KumarAinda não há avaliações
- Abdominoperineal ResectionDocumento17 páginasAbdominoperineal ResectionOhana S.Ainda não há avaliações
- Dr. Pranaya Kumar Panigrahi: PG StudentDocumento104 páginasDr. Pranaya Kumar Panigrahi: PG Studentprabowoaji12Ainda não há avaliações
- CholecystectomyDocumento2 páginasCholecystectomyHiylie MartinezAinda não há avaliações
- The Ileoanal Pouch: A Practical Guide for Surgery, Management and TroubleshootingNo EverandThe Ileoanal Pouch: A Practical Guide for Surgery, Management and TroubleshootingJanindra WarusavitarneAinda não há avaliações
- Difficult Acute Cholecystitis: Treatment and Technical IssuesNo EverandDifficult Acute Cholecystitis: Treatment and Technical IssuesAinda não há avaliações
- A Manual of the Operations of Surgery: For the Use of Senior Students, House Surgeons, and Junior PractitionersNo EverandA Manual of the Operations of Surgery: For the Use of Senior Students, House Surgeons, and Junior PractitionersAinda não há avaliações
- Los Terrybles Book TeamDocumento6 páginasLos Terrybles Book TeamWildor Herrera GuevaraAinda não há avaliações
- Colectomia Izquierda, Anastomosis Termino-TerminalDocumento11 páginasColectomia Izquierda, Anastomosis Termino-TerminalWildor Herrera GuevaraAinda não há avaliações
- Los Terrybles Book TeamDocumento10 páginasLos Terrybles Book TeamWildor Herrera GuevaraAinda não há avaliações
- Cirugia Anatomica Del Intestino GruesoDocumento3 páginasCirugia Anatomica Del Intestino GruesoWildor Herrera GuevaraAinda não há avaliações
- Los Terrybles Book TeamDocumento6 páginasLos Terrybles Book TeamWildor Herrera GuevaraAinda não há avaliações
- Cierre de ColostomiaDocumento9 páginasCierre de ColostomiaWildor Herrera GuevaraAinda não há avaliações
- Los Terrybles Book TeamDocumento14 páginasLos Terrybles Book TeamWildor Herrera GuevaraAinda não há avaliações
- Anastomosis de Colon Con GrapasDocumento5 páginasAnastomosis de Colon Con GrapasWildor Herrera GuevaraAinda não há avaliações
- Anatomia Y Resecciones de HigadoDocumento4 páginasAnatomia Y Resecciones de HigadoWildor Herrera GuevaraAinda não há avaliações
- User'S Guide: Tm4C Series Tm4C129E Crypto Connected Launchpad Evaluation KitDocumento36 páginasUser'S Guide: Tm4C Series Tm4C129E Crypto Connected Launchpad Evaluation KitLương Văn HưởngAinda não há avaliações
- Worlds Apart: A Story of Three Possible Warmer WorldsDocumento1 páginaWorlds Apart: A Story of Three Possible Warmer WorldsJuan Jose SossaAinda não há avaliações
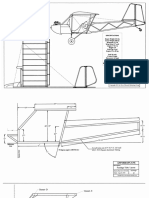
- Plans PDFDocumento49 páginasPlans PDFEstevam Gomes de Azevedo85% (34)
- EXP4 The Diels Alder ReactionsDocumento3 páginasEXP4 The Diels Alder ReactionsLaura GuidoAinda não há avaliações
- Fulltext 4 PDFDocumento4 páginasFulltext 4 PDFSubhadip Banerjee0% (1)
- Catalogo GatesDocumento255 páginasCatalogo GatesBenjamin HedoneweAinda não há avaliações
- Recipes From The Perfect Scoop by David LebovitzDocumento10 páginasRecipes From The Perfect Scoop by David LebovitzThe Recipe Club100% (7)
- Ad149 Manual RDocumento69 páginasAd149 Manual RCharityAinda não há avaliações
- MarbiehistoryDocumento6 páginasMarbiehistoryMarbie DalanginAinda não há avaliações
- Managing Diabetic Foot Ulcers ReadingDocumento21 páginasManaging Diabetic Foot Ulcers Readinghimanshugupta811997Ainda não há avaliações
- Combined Shear and TensionDocumento16 páginasCombined Shear and TensionDAN MARK OPONDAAinda não há avaliações
- Guia de CondensadoresDocumento193 páginasGuia de CondensadoresPaola Segura CorreaAinda não há avaliações
- Standard Cost EstimateDocumento21 páginasStandard Cost EstimateMOORTHYAinda não há avaliações
- Middle Range Theory Ellen D. Schulzt: Modeling and Role Modeling Katharine Kolcaba: Comfort TheoryDocumento22 páginasMiddle Range Theory Ellen D. Schulzt: Modeling and Role Modeling Katharine Kolcaba: Comfort TheoryMerlinAinda não há avaliações
- Purpose in LifeDocumento1 páginaPurpose in Lifeaashish95100% (1)
- Electrowetting - Wikipedia, The Free EncyclopediaDocumento5 páginasElectrowetting - Wikipedia, The Free EncyclopediaDwane AlmeidaAinda não há avaliações
- 3200AMMe - Part 4Documento207 páginas3200AMMe - Part 4Tanja Kesic100% (1)
- American BreakfastDocumento4 páginasAmerican BreakfastHamilton Valenzuela ChipongianAinda não há avaliações
- TNM History Updated June2017Documento2 páginasTNM History Updated June2017Lucas AndreoAinda não há avaliações
- AssessmentDocumento3 páginasAssessmentpalflaxAinda não há avaliações
- DudjDocumento4 páginasDudjsyaiful rinantoAinda não há avaliações
- Eng DS Epp-2314 1410Documento2 páginasEng DS Epp-2314 1410MarkusAldoMaquAinda não há avaliações
- Passenger Lift Alert - Health and Safety AuthorityDocumento4 páginasPassenger Lift Alert - Health and Safety AuthorityReginald MaswanganyiAinda não há avaliações
- FemDocumento4 páginasFemAditya SharmaAinda não há avaliações
- Someone Who Believes in YouDocumento1 páginaSomeone Who Believes in YouMANOLO C. LUCENECIOAinda não há avaliações
- Fundamentals of Pain Medicine: Jianguo Cheng Richard W. RosenquistDocumento346 páginasFundamentals of Pain Medicine: Jianguo Cheng Richard W. RosenquistMayAinda não há avaliações
- Straight LineDocumento15 páginasStraight LineAyanAinda não há avaliações
- TM-8000 HD Manual PDFDocumento37 páginasTM-8000 HD Manual PDFRoxana BirtumAinda não há avaliações
- Gamak MotorDocumento34 páginasGamak MotorCengiz Sezer100% (1)
- Cynosure Starlux 500 Palomar Technical Service ManualDocumento47 páginasCynosure Starlux 500 Palomar Technical Service ManualJF SilvaAinda não há avaliações