Você também pode gostar
- Difficulty in Speech After StrokeDocumento6 páginasDifficulty in Speech After StrokeAJ RegaladoAinda não há avaliações
- Carbuncle, Incision, Drainage, DebridementDocumento11 páginasCarbuncle, Incision, Drainage, DebridementAlvin Germo PasuquinAinda não há avaliações
- Case Presentation IM DDHDocumento12 páginasCase Presentation IM DDHAishwarya BharathAinda não há avaliações
- Protocol - IM DyspneaDocumento7 páginasProtocol - IM DyspneaTrisAinda não há avaliações
- Pancytopenia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandPancytopenia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- Dizziness and Difficulty Breathing CaseDocumento4 páginasDizziness and Difficulty Breathing CaseLucyellowOttemoesoeAinda não há avaliações
- Case ReportDocumento19 páginasCase ReportvivitaslimAinda não há avaliações
- Collin Grimes Patient Write Up June 14Documento4 páginasCollin Grimes Patient Write Up June 14CollinAinda não há avaliações
- Medical Case 1: Language Centre of Malahayati University at 2010Documento16 páginasMedical Case 1: Language Centre of Malahayati University at 2010putri1114Ainda não há avaliações
- Surgery Case AppendicitisDocumento30 páginasSurgery Case AppendicitisSarahAinda não há avaliações
- Asthma Patient ProfileDocumento8 páginasAsthma Patient ProfileGlenn Asuncion PagaduanAinda não há avaliações
- Disturbances in Respiratory FunctionDocumento6 páginasDisturbances in Respiratory FunctionSeff CausapinAinda não há avaliações
- Case Presentation - GASTRODocumento46 páginasCase Presentation - GASTROalidudeAinda não há avaliações
- Bronchial Asthma (1) SKDocumento24 páginasBronchial Asthma (1) SKSafoora RafeeqAinda não há avaliações
- Internal Medicine Case Write Up 1Documento14 páginasInternal Medicine Case Write Up 1Roshandiep GillAinda não há avaliações
- Endocrine Long CaseDocumento8 páginasEndocrine Long CaseNadia SalwaniAinda não há avaliações
- Case Study On Jaundice With AnswersDocumento4 páginasCase Study On Jaundice With Answersabirami pAinda não há avaliações
- Reye's SyndromeDocumento11 páginasReye's SyndromeChristine Go100% (1)
- Case Write-Up 1 Obstructive Jaundice With Cholecystitis Secondary To Ampullary TumorDocumento21 páginasCase Write-Up 1 Obstructive Jaundice With Cholecystitis Secondary To Ampullary TumorwhosenahAinda não há avaliações
- Cirrhosis Case For PrintingDocumento12 páginasCirrhosis Case For PrintingSean Mercado100% (1)
- History TakingDocumento9 páginasHistory TakingMaria Santiago100% (2)
- CASE 2 PneumoniaDocumento12 páginasCASE 2 PneumoniaKenneth MiguelAinda não há avaliações
- Surgery 2 Case ReportDocumento12 páginasSurgery 2 Case ReportElvis NgAinda não há avaliações
- Internal Medicine Write Up 1Documento16 páginasInternal Medicine Write Up 1Ariff MahdzubAinda não há avaliações
- (IM Ward) History Taking Tool PDFDocumento15 páginas(IM Ward) History Taking Tool PDFleapacis100% (1)
- Pud Case StudyDocumento8 páginasPud Case Studyapi-346620455Ainda não há avaliações
- Derain Carla Elize-Group9 DXRDocumento6 páginasDerain Carla Elize-Group9 DXRCarla Elize Derain100% (1)
- Liver Disease in 30-Year-Old FarmerDocumento5 páginasLiver Disease in 30-Year-Old FarmerKanwaljeet SinghAinda não há avaliações
- Record The Patient's VATEF: Based On The Data ProvidedDocumento19 páginasRecord The Patient's VATEF: Based On The Data ProvidedRakesh KumarAinda não há avaliações
- AsthmaDocumento39 páginasAsthmamits98Ainda não há avaliações
- Pulmonology Case Presentation on COPD ExacerbationDocumento20 páginasPulmonology Case Presentation on COPD ExacerbationMohamad HafyfyAinda não há avaliações
- Bronchial Asthma GuideDocumento59 páginasBronchial Asthma GuideJb TlntinoAinda não há avaliações
- National Guidelines On Management of Dengue Fever & Dengue Haemorrhagic Fever in Children and Adolescents - Sri LankaDocumento53 páginasNational Guidelines On Management of Dengue Fever & Dengue Haemorrhagic Fever in Children and Adolescents - Sri LankaNational Dengue Control Unit,Sri Lanka100% (1)
- Insulin and Oral Hypoglycemic DrugsDocumento30 páginasInsulin and Oral Hypoglycemic DrugsAngga NugrahaAinda não há avaliações
- Pedia - DengueDocumento10 páginasPedia - DengueJan Mikhail FrascoAinda não há avaliações
- Cor Pulmonale PresentationDocumento17 páginasCor Pulmonale Presentationandi reskifaisAinda não há avaliações
- Case PresentationDocumento5 páginasCase Presentationahmadhajjj100% (1)
- Pat 2 Medsurg1Documento20 páginasPat 2 Medsurg1api-300849832Ainda não há avaliações
- Opd CaseDocumento13 páginasOpd CaseRaven CièlAinda não há avaliações
- Grand ReportsDocumento60 páginasGrand ReportsfilchibuffAinda não há avaliações
- A Case Study Of: Hypertension Emergency, Hypertensive Cardiovascular DiseaseDocumento23 páginasA Case Study Of: Hypertension Emergency, Hypertensive Cardiovascular DiseaseKristine AlejandroAinda não há avaliações
- My Cwu OphthalDocumento16 páginasMy Cwu OphthalSalsabila Al-BasheerAinda não há avaliações
- Background: Viral Mumps InfectionDocumento5 páginasBackground: Viral Mumps InfectionAgustin UyAinda não há avaliações
- Case Study on Managing a Pediatric Femur FractureDocumento29 páginasCase Study on Managing a Pediatric Femur FractureEden CruzAinda não há avaliações
- Nursing Process 3Documento10 páginasNursing Process 3Shubhra Sheoran100% (1)
- IM AdconDocumento28 páginasIM AdconCla SantosAinda não há avaliações
- Case Presentation On Copd: By, Thomas Eipe Pharm D InternDocumento32 páginasCase Presentation On Copd: By, Thomas Eipe Pharm D InternThomas EipeAinda não há avaliações
- Internal Medicine Case PresentationDocumento114 páginasInternal Medicine Case PresentationAyen FornollesAinda não há avaliações
- Pa Tool MihpDocumento23 páginasPa Tool MihpNassif M. BangcolaAinda não há avaliações
- Pediatrics 2 LaboratoryDocumento40 páginasPediatrics 2 LaboratoryAmaetenAinda não há avaliações
- ICU Case: Septic Shock from Hospital-Acquired PneumoniaDocumento13 páginasICU Case: Septic Shock from Hospital-Acquired PneumoniaHana FauziAinda não há avaliações
- Pediatric Case Presentation 1Documento18 páginasPediatric Case Presentation 1Laica BarcelonaAinda não há avaliações
- Case report of 3-year old boy with asthmaDocumento6 páginasCase report of 3-year old boy with asthmaJiaYee GoAinda não há avaliações
- Shivaani (Internal Medicine CWU)Documento12 páginasShivaani (Internal Medicine CWU)S.M. Manogaran Shivaani AP S.M. ManogaranAinda não há avaliações
- Pediatrics History and Physical ExamDocumento16 páginasPediatrics History and Physical ExamstarrnewmanpaAinda não há avaliações
- CVA Case PresentationDocumento16 páginasCVA Case PresentationgolokipokAinda não há avaliações
- History TakingDocumento28 páginasHistory TakingguldonAinda não há avaliações
- Physical Examination: Binal Joshi Assistant Professor Child Health Nursing Manikaka Topawala Institute of NursingDocumento101 páginasPhysical Examination: Binal Joshi Assistant Professor Child Health Nursing Manikaka Topawala Institute of NursingBinal JoshiAinda não há avaliações
- MT 1 Combined Top 200Documento3 páginasMT 1 Combined Top 200ShohanAinda não há avaliações
- Revision Summary - Rainbow's End by Jane Harrison PDFDocumento47 páginasRevision Summary - Rainbow's End by Jane Harrison PDFchris100% (3)
- 25 Virtues Explained with Real Life SituationsDocumento5 páginas25 Virtues Explained with Real Life Situationsleslie vine deloso100% (2)
- Perancangan Kota: Jurusan Perencanaan Wilayah Dan Kota Institut Teknologi Nasional Tahun 2021/2022Documento27 páginasPerancangan Kota: Jurusan Perencanaan Wilayah Dan Kota Institut Teknologi Nasional Tahun 2021/2022idaAinda não há avaliações
- Business Beyond Profit Motivation Role of Employees As Decision-Makers in The Business EnterpriseDocumento6 páginasBusiness Beyond Profit Motivation Role of Employees As Decision-Makers in The Business EnterpriseCaladhiel100% (1)
- Indian Medicinal PlantsDocumento121 páginasIndian Medicinal PlantsN S Arun KumarAinda não há avaliações
- The Political Philosophy of Giorgio Agamben A Critical EvaluationDocumento20 páginasThe Political Philosophy of Giorgio Agamben A Critical EvaluationLEAAinda não há avaliações
- Installation, Operation and Maintenance Instructions Stainless Steel, Liquid Ring Vacuum PumpsDocumento28 páginasInstallation, Operation and Maintenance Instructions Stainless Steel, Liquid Ring Vacuum PumpspinplataAinda não há avaliações
- The Greco-Turkish War of 1920-1922: Greece Seeks Territory in Asia MinorDocumento14 páginasThe Greco-Turkish War of 1920-1922: Greece Seeks Territory in Asia MinorFauzan Rasip100% (1)
- ZZXCDocumento2 páginasZZXCKrisleen AbrenicaAinda não há avaliações
- Exp Mun Feb-15 (Excel)Documento7.510 páginasExp Mun Feb-15 (Excel)Vivek DomadiaAinda não há avaliações
- Symbian Os-Seminar ReportDocumento20 páginasSymbian Os-Seminar Reportitsmemonu100% (1)
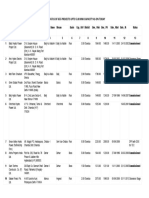
- List/Status of 655 Projects Upto 5.00 MW Capacity As On TodayDocumento45 páginasList/Status of 655 Projects Upto 5.00 MW Capacity As On Todayganvaqqqzz21Ainda não há avaliações
- Sleeping Habits: HH Mahanidhi SwamiDocumento3 páginasSleeping Habits: HH Mahanidhi SwamiJeevanAinda não há avaliações
- AC & Crew Lists 881st 5-18-11Documento43 páginasAC & Crew Lists 881st 5-18-11ywbh100% (2)
- Timpuri Verbale Engleza RezumatDocumento5 páginasTimpuri Verbale Engleza RezumatBogdan StefanAinda não há avaliações
- Carbon Footprint AnalysisDocumento18 páginasCarbon Footprint AnalysisAndres AndradeAinda não há avaliações
- KARTONAN PRODUkDocumento30 páginasKARTONAN PRODUkAde SeprialdiAinda não há avaliações
- Accounting What The Numbers Mean 11th Edition Marshall Solutions Manual 1Documento36 páginasAccounting What The Numbers Mean 11th Edition Marshall Solutions Manual 1amandawilkinsijckmdtxez100% (23)
- Minsc and Boo's Journal of VillainyDocumento158 páginasMinsc and Boo's Journal of VillainyAPCommentator100% (1)
- Thecodeblocks Com Acl in Nodejs ExplainedDocumento1 páginaThecodeblocks Com Acl in Nodejs ExplainedHamza JaveedAinda não há avaliações
- Is The Question Too Broad or Too Narrow?Documento3 páginasIs The Question Too Broad or Too Narrow?teo100% (1)
- The Wavy Tunnel: Trade Management Jody SamuelsDocumento40 páginasThe Wavy Tunnel: Trade Management Jody SamuelsPeter Nguyen100% (1)
- NDA Template Non Disclosure Non Circumvent No Company NameDocumento9 páginasNDA Template Non Disclosure Non Circumvent No Company NamepvorsterAinda não há avaliações
- (Click Here) : Watch All Paid Porn Sites For FreeDocumento16 páginas(Click Here) : Watch All Paid Porn Sites For Freexboxlivecode2011Ainda não há avaliações
- Marylebone Construction UpdateDocumento2 páginasMarylebone Construction UpdatePedro SousaAinda não há avaliações
- Powerpoint Lectures For Principles of Macroeconomics, 9E by Karl E. Case, Ray C. Fair & Sharon M. OsterDocumento24 páginasPowerpoint Lectures For Principles of Macroeconomics, 9E by Karl E. Case, Ray C. Fair & Sharon M. OsterJiya Nitric AcidAinda não há avaliações
- 2020052336Documento4 páginas2020052336Kapil GurunathAinda não há avaliações
- Teacher swap agreement for family reasonsDocumento4 páginasTeacher swap agreement for family reasonsKimber LeeAinda não há avaliações
- El Rol Del Fonoaudiólogo Como Agente de Cambio Social (Segundo Borrador)Documento11 páginasEl Rol Del Fonoaudiólogo Como Agente de Cambio Social (Segundo Borrador)Jorge Nicolás Silva Flores100% (1)