Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Sample Questionnaire: Stanford Patient Education Research CenterDocumento8 páginasSample Questionnaire: Stanford Patient Education Research CenterKamalakannanSwasthAinda não há avaliações
- Aha Acls Prep Packet 2020Documento69 páginasAha Acls Prep Packet 2020VP The Hacker100% (2)
- Preventing LonelinessDocumento16 páginasPreventing LonelinessshutekiAinda não há avaliações
- Echocardiography Evaluation For The Tricuspid ValveDocumento48 páginasEchocardiography Evaluation For The Tricuspid ValveSofia KusumadewiAinda não há avaliações
- Heart Sounds: They Are The Sounds Produced by The Mechanical Activities of The Heart During Each Cadiac CycleDocumento19 páginasHeart Sounds: They Are The Sounds Produced by The Mechanical Activities of The Heart During Each Cadiac Cyclevishnudurga100% (1)
- Cardiac Resynchronization Therapy (Sep 19 2007) - (1841846376) - (CRC Press)Documento337 páginasCardiac Resynchronization Therapy (Sep 19 2007) - (1841846376) - (CRC Press)Morozovschi VitalieAinda não há avaliações
- ECG Changes in Drug and Electrolyte AbnormalitiesDocumento28 páginasECG Changes in Drug and Electrolyte AbnormalitiesNachiket Vijay PotdarAinda não há avaliações
- Hypoglychemia AdultsDocumento32 páginasHypoglychemia AdultsshutekiAinda não há avaliações
- Food and Drug Interactions: Recent NewsDocumento6 páginasFood and Drug Interactions: Recent NewsshutekiAinda não há avaliações
- Con Dem and DepDocumento23 páginasCon Dem and DepshutekiAinda não há avaliações
- Domain 5Documento1 páginaDomain 5shutekiAinda não há avaliações
- Sayed Jurnal 1Documento13 páginasSayed Jurnal 1Reynaldo AffandiAinda não há avaliações
- Serve and ReturnDocumento1 páginaServe and ReturnshutekiAinda não há avaliações
- QapiDocumento5 páginasQapishutekiAinda não há avaliações
- Con Dem and DepDocumento23 páginasCon Dem and DepshutekiAinda não há avaliações
- RA Treatment 2009Documento5 páginasRA Treatment 2009shutekiAinda não há avaliações
- ADTI SMMSE-GDS Reference Card PDFDocumento2 páginasADTI SMMSE-GDS Reference Card PDFSummer WrightAinda não há avaliações
- T3 CECMHCInfantDocumento2 páginasT3 CECMHCInfantshutekiAinda não há avaliações
- ADTI SMMSE-GDS Reference Card PDFDocumento2 páginasADTI SMMSE-GDS Reference Card PDFSummer WrightAinda não há avaliações
- Kontraktur AnakDocumento10 páginasKontraktur AnakshutekiAinda não há avaliações
- Oleh: Dra. Junaiti Sahar, PHD Fik Ui: Reproductive and Sexuality in Older PersonDocumento32 páginasOleh: Dra. Junaiti Sahar, PHD Fik Ui: Reproductive and Sexuality in Older PersonshutekiAinda não há avaliações
- Kontraktur AnakDocumento10 páginasKontraktur AnakshutekiAinda não há avaliações
- GoutDocumento36 páginasGoutshutekiAinda não há avaliações
- Meeting The Nutrition Needs of ElderlyDocumento1 páginaMeeting The Nutrition Needs of ElderlyshutekiAinda não há avaliações
- PCDocumento2 páginasPCshutekiAinda não há avaliações
- Kontraktur AnakDocumento10 páginasKontraktur AnakshutekiAinda não há avaliações
- CitationsDocumento9 páginasCitationsanil_049Ainda não há avaliações
- Premature Infant Pain Profile (PIPP) : Indicator Finding PointsDocumento2 páginasPremature Infant Pain Profile (PIPP) : Indicator Finding PointsshutekiAinda não há avaliações
- Self ReflectionDocumento1 páginaSelf ReflectionshutekiAinda não há avaliações
- IEHCDocumento13 páginasIEHCshutekiAinda não há avaliações
- AAOHN StandardsDocumento3 páginasAAOHN StandardsshutekiAinda não há avaliações
- CDC PriorDocumento8 páginasCDC PriorshutekiAinda não há avaliações
- CDC PriorDocumento8 páginasCDC PriorshutekiAinda não há avaliações
- Breathing Exercises: Purpose PolicyDocumento5 páginasBreathing Exercises: Purpose PolicyshutekiAinda não há avaliações
- Diastolic CHF DiagnosisDocumento3 páginasDiastolic CHF DiagnosissamAinda não há avaliações
- Evaluacion Valvula MitralDocumento9 páginasEvaluacion Valvula MitralRafaelDavidVillalbaRodriguezAinda não há avaliações
- Cardiac Disorders in ChildrenDocumento41 páginasCardiac Disorders in ChildrenB AuAinda não há avaliações
- BagusDocumento10 páginasBagusBelinda SuhuyanlyAinda não há avaliações
- Schedule D: List of Life Saveing or Life Sustaining Medical DevicesDocumento5 páginasSchedule D: List of Life Saveing or Life Sustaining Medical DevicesAasma RehmanAinda não há avaliações
- Pengaruh Kompresi RJP Dengan Metronom Terhadap Kualitas Kompresi RJP Yang Dilakukan Mahasiswa PerawatDocumento7 páginasPengaruh Kompresi RJP Dengan Metronom Terhadap Kualitas Kompresi RJP Yang Dilakukan Mahasiswa PerawatGabriela Adeleda LeiwakabessyAinda não há avaliações
- Procedure For DefibrillationDocumento6 páginasProcedure For DefibrillationTasia DeastutiAinda não há avaliações
- 19 Cardiac DisordersDocumento51 páginas19 Cardiac DisordersChessie Garcia100% (1)
- PHA Accredited Institutions June 2021Documento9 páginasPHA Accredited Institutions June 2021JoyAinda não há avaliações
- ACLS Drug Therapy RevisedDocumento4 páginasACLS Drug Therapy RevisedpaveethrahAinda não há avaliações
- NCMB 312 Lec Course Task CU2: Our Lady of Fatima UniversityDocumento2 páginasNCMB 312 Lec Course Task CU2: Our Lady of Fatima UniversityMushy_ayaAinda não há avaliações
- Heart Failure: Dr.K.Sathish Kumar, MD (Hom) .Documento11 páginasHeart Failure: Dr.K.Sathish Kumar, MD (Hom) .mnr hmcAinda não há avaliações
- TOF in AdultDocumento26 páginasTOF in AdultsalsaAinda não há avaliações
- Dr. Suryono - NSTEMI What We Can Learn From GRACE and TIMIDocumento21 páginasDr. Suryono - NSTEMI What We Can Learn From GRACE and TIMIDilaAinda não há avaliações
- Drugs in CHFDocumento48 páginasDrugs in CHFBishnu BhandariAinda não há avaliações
- AHA Guideline NSTEMI 2014 PDFDocumento71 páginasAHA Guideline NSTEMI 2014 PDFkiyoeugraAinda não há avaliações
- Susila Wahiddiyah, Alfi Ari Fahrul RizalDocumento10 páginasSusila Wahiddiyah, Alfi Ari Fahrul RizalNandha PuspitaSariAinda não há avaliações
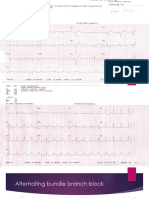
- Alternating Bundle Branch BlockDocumento9 páginasAlternating Bundle Branch BlockSyifa Mahmud Syukran AkbarAinda não há avaliações
- Nephrotic Syndrome Nephritic SyndromeDocumento3 páginasNephrotic Syndrome Nephritic Syndromekvs gouthamAinda não há avaliações
- High-Sensitivity Cardiac Troponin at Presentation To Rule Out Myocardial Infarction (Historic)Documento20 páginasHigh-Sensitivity Cardiac Troponin at Presentation To Rule Out Myocardial Infarction (Historic)DenisseRangelAinda não há avaliações
- eGFR - Estimated Glomerular Filtration RateDocumento3 páginaseGFR - Estimated Glomerular Filtration RateDiane JoyceAinda não há avaliações
- List of Registrable Postgraduate Medical QualificationsDocumento5 páginasList of Registrable Postgraduate Medical QualificationsAchwani SantoshAinda não há avaliações
- ECG at A GlanceDocumento53 páginasECG at A Glancenurliah armandAinda não há avaliações
- SymptomatologyDocumento2 páginasSymptomatologyAyaBasilioAinda não há avaliações
- Kidney Disease Community Health PresentationDocumento17 páginasKidney Disease Community Health PresentationVanessa FloresAinda não há avaliações