Você também pode gostar
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Nyeri PayudaraDocumento11 páginasNyeri PayudaraRezy Arina PutriAinda não há avaliações
- 1000,1090+,1100,1105 Scanner User Guide - v3.02Documento46 páginas1000,1090+,1100,1105 Scanner User Guide - v3.02Rezy Arina PutriAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Psikologi Memori Emosional PDFDocumento13 páginasPsikologi Memori Emosional PDFInggridCliquersAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Rita Purnama Sari Ygo Jurnal.Documento8 páginasRita Purnama Sari Ygo Jurnal.Fausiah Ulva MAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- 2012 664593Documento17 páginas2012 664593Rezy Arina PutriAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Ipi 179256Documento7 páginasIpi 179256Rezy Arina PutriAinda não há avaliações
- Dody Novrial 9Documento15 páginasDody Novrial 9Rezy Arina PutriAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Holmes Gathercvole Ed Psych 2013Documento13 páginasHolmes Gathercvole Ed Psych 2013Rezy Arina PutriAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Psikologi Memori Emosional PDFDocumento13 páginasPsikologi Memori Emosional PDFInggridCliquersAinda não há avaliações
- Ipi 179256Documento7 páginasIpi 179256Rezy Arina PutriAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- Holmes Gathercvole Ed Psych 2013Documento13 páginasHolmes Gathercvole Ed Psych 2013Rezy Arina PutriAinda não há avaliações
- 2013 - Is Working Memory Training Effective - A Meta-Analytic Review PDFDocumento22 páginas2013 - Is Working Memory Training Effective - A Meta-Analytic Review PDFAída MoraAinda não há avaliações
- 2013 - Is Working Memory Training Effective - A Meta-Analytic Review PDFDocumento22 páginas2013 - Is Working Memory Training Effective - A Meta-Analytic Review PDFAída MoraAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- 351 1306 1 PBDocumento18 páginas351 1306 1 PBRezy Arina PutriAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- 181 355 1 PBDocumento6 páginas181 355 1 PBRezy Arina PutriAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Holmes Gathercvole Ed Psych 2013Documento13 páginasHolmes Gathercvole Ed Psych 2013Rezy Arina PutriAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Vol - 3 - No - 1 - B - Hubungan Pengetahuan Ibu Tentang Gizi Dengan Perkembangan Kognitif Anak Usia 24-59 BulanDocumento6 páginasVol - 3 - No - 1 - B - Hubungan Pengetahuan Ibu Tentang Gizi Dengan Perkembangan Kognitif Anak Usia 24-59 BulanRezy Arina PutriAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- Nyeri PayudaraDocumento11 páginasNyeri PayudaraRezy Arina PutriAinda não há avaliações
- 9086 25868 1 SM PDFDocumento8 páginas9086 25868 1 SM PDFRezy Arina PutriAinda não há avaliações
- BelimbingDocumento12 páginasBelimbingMuhammad AlfianAinda não há avaliações
- Hubungan Kecukupan Asam Eikosapentanoat (Epa), Asam Dokosaheksanoat (Dha) Ikan Dan Status Gizi Dengan Prestasi Belajar SiswaDocumento11 páginasHubungan Kecukupan Asam Eikosapentanoat (Epa), Asam Dokosaheksanoat (Dha) Ikan Dan Status Gizi Dengan Prestasi Belajar SiswaRezy Arina PutriAinda não há avaliações
- Hubungan Kecukupan Asam Eikosapentanoat (Epa), Asam Dokosaheksanoat (Dha) Ikan Dan Status Gizi Dengan Prestasi Belajar SiswaDocumento11 páginasHubungan Kecukupan Asam Eikosapentanoat (Epa), Asam Dokosaheksanoat (Dha) Ikan Dan Status Gizi Dengan Prestasi Belajar SiswaRezy Arina PutriAinda não há avaliações
- The Relation of Husband'S Support and Breastfeeding Production Postpartum Maternal in Puskesmas Senori TubanDocumento13 páginasThe Relation of Husband'S Support and Breastfeeding Production Postpartum Maternal in Puskesmas Senori Tubanrudy_77Ainda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Efektifitas Kombinasi Terapi Kukusan Labu Siam dan Senam Anti Stroke untuk Mengurangi Tekanan Darah pada HipertensiDocumento9 páginasEfektifitas Kombinasi Terapi Kukusan Labu Siam dan Senam Anti Stroke untuk Mengurangi Tekanan Darah pada HipertensiRezy Arina PutriAinda não há avaliações
- Nyeri PayudaraDocumento11 páginasNyeri PayudaraRezy Arina PutriAinda não há avaliações
- Pisang Terhadap HipertensiDocumento6 páginasPisang Terhadap HipertensiRezy Arina PutriAinda não há avaliações
- Pjat TanganDocumento6 páginasPjat TanganRezy Arina PutriAinda não há avaliações
- Pjat TanganDocumento6 páginasPjat TanganRezy Arina PutriAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Jurnal SafetyDocumento11 páginasJurnal SafetyRezy Arina PutriAinda não há avaliações
- Mendelian Genetics and ExtensionsDocumento39 páginasMendelian Genetics and ExtensionskcqywAinda não há avaliações
- Structure and Function of The OvariesDocumento3 páginasStructure and Function of The OvariesAnonymous FfdoEXAinda não há avaliações
- Booklet, Vol 10, No 3, September 2020Documento154 páginasBooklet, Vol 10, No 3, September 2020evelAinda não há avaliações
- Animal BiotechnologyDocumento50 páginasAnimal BiotechnologyJyotsna Ravikumar60% (10)
- First Grading Advance Science Reviewer Grade 7Documento7 páginasFirst Grading Advance Science Reviewer Grade 7loraineAinda não há avaliações
- W. James Kent - BLAT-The BLAST-Like Alignment ToolDocumento10 páginasW. James Kent - BLAT-The BLAST-Like Alignment ToolYopghm698Ainda não há avaliações
- Nutrition in Plants Class 7 Science NotesDocumento4 páginasNutrition in Plants Class 7 Science NotesshravandownloadAinda não há avaliações
- 10 DNA Testing Myths Busted, and Other Favorite Posts: by Blaine T. BettingerDocumento11 páginas10 DNA Testing Myths Busted, and Other Favorite Posts: by Blaine T. BettingerSexy888Ainda não há avaliações
- Mitosis PowerpointDocumento31 páginasMitosis PowerpointLeenfranzen MagadiaAinda não há avaliações
- European Journal of PharmacologyDocumento13 páginasEuropean Journal of Pharmacologykamal.nayanAinda não há avaliações
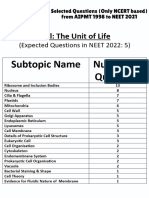
- Cell - The Unit of Life - NCERT Based PYQsDocumento9 páginasCell - The Unit of Life - NCERT Based PYQsAkhil singhAinda não há avaliações
- Nervous System Test QuestionsDocumento2 páginasNervous System Test QuestionsRox Francisco100% (3)
- IL-17 and TBDocumento10 páginasIL-17 and TBchhatraAinda não há avaliações
- 3rd GRADING PERIODICAL EXAM MAPEH 8Documento1 página3rd GRADING PERIODICAL EXAM MAPEH 8Amor BatasAinda não há avaliações
- Tunza 2009 Youth Conferences - What We Want From CopenhagenDocumento24 páginasTunza 2009 Youth Conferences - What We Want From CopenhagenUnited Nations Environment ProgrammeAinda não há avaliações
- Bio Practicals 2022-23Documento31 páginasBio Practicals 2022-23Aman AaryanAinda não há avaliações
- Preventive Veterinary Medicine PDFDocumento48 páginasPreventive Veterinary Medicine PDFMasum Rana100% (2)
- Wound Healing: Healing by First Intention (Primary Union)Documento31 páginasWound Healing: Healing by First Intention (Primary Union)Muhammad Masoom AkhtarAinda não há avaliações
- Resources 11 00015 v2Documento20 páginasResources 11 00015 v2Gina M LópezAinda não há avaliações
- Pneumocystis Cariinii 1Documento13 páginasPneumocystis Cariinii 1Tharsini SalyamAinda não há avaliações
- G9 Science Q1 Week 3 4 Non Mendelian Patterns of InheritanDocumento26 páginasG9 Science Q1 Week 3 4 Non Mendelian Patterns of InheritanSandra Lee LigsaAinda não há avaliações
- LESSON PLAN Food Chains and Food Webs - AFT - Putri Dyah Astari (Quiz Only)Documento13 páginasLESSON PLAN Food Chains and Food Webs - AFT - Putri Dyah Astari (Quiz Only)AfnestyaAinda não há avaliações
- Agricultural MicrobiologyDocumento256 páginasAgricultural MicrobiologyJay JayakumarAinda não há avaliações
- The association between acute asthma severity and peripheral blood inflammatory cellsDocumento6 páginasThe association between acute asthma severity and peripheral blood inflammatory cellsFarel Muhammad Sayyaf HaydarAinda não há avaliações
- New Zealand White Rabbits: Model Information SheetDocumento2 páginasNew Zealand White Rabbits: Model Information SheetVermilion~Ainda não há avaliações
- Thalassemia WikiDocumento12 páginasThalassemia Wikiholy_miracleAinda não há avaliações
- Module 9 - Earth & Life ScienceDocumento25 páginasModule 9 - Earth & Life ScienceRosalyn Marie Sugay64% (14)
- 1962, Waddington, How Animals DevelopDocumento148 páginas1962, Waddington, How Animals DevelopLuis Ossa FuentesAinda não há avaliações
- Activity No. 3: Structure of A Cell and MitosisDocumento9 páginasActivity No. 3: Structure of A Cell and MitosisEricka GenoveAinda não há avaliações
- Genetic EngineeringDocumento43 páginasGenetic EngineeringGeonyzl L. AlviolaAinda não há avaliações
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNo EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNota: 4 de 5 estrelas4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityNo EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityNota: 4 de 5 estrelas4/5 (13)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNo EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNota: 3.5 de 5 estrelas3.5/5 (3)
- Why We Die: The New Science of Aging and the Quest for ImmortalityNo EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityNota: 3.5 de 5 estrelas3.5/5 (2)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNo EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNota: 5 de 5 estrelas5/5 (78)