Você também pode gostar
- 2020.06.09 Federal Complaint FinalsignedDocumento27 páginas2020.06.09 Federal Complaint Finalsignedwtopweb100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Loudoun County Teacher Salary PlanDocumento2 páginasLoudoun County Teacher Salary PlanwtopwebAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
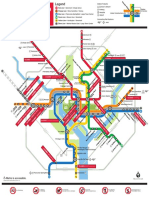
- 2019 System Map COVID-19 Stations FINALDocumento1 página2019 System Map COVID-19 Stations FINALwtopwebAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- DC Police Seek Persons of InterestDocumento140 páginasDC Police Seek Persons of InterestwtopwebAinda não há avaliações
- Gonzales Maryland Poll Report January 2020Documento29 páginasGonzales Maryland Poll Report January 2020wtopwebAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Michael Gerhardt's Opening StatementDocumento10 páginasMichael Gerhardt's Opening StatementStefan BecketAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Pamela Karlan's Opening StatementDocumento6 páginasPamela Karlan's Opening StatementStefan BecketAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Chesapeake Bay Crossing StudyDocumento4 páginasChesapeake Bay Crossing StudywtopwebAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Read Turley TestimonyDocumento53 páginasRead Turley Testimonykballuck186% (7)
- Feldman TestimonyDocumento6 páginasFeldman TestimonyGeoffrey Rowland100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Catherine Pugh IndictmentDocumento34 páginasCatherine Pugh IndictmentWJZAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Jack Evans' Attorneys Respond To O'Melveny-Myers ReportDocumento67 páginasJack Evans' Attorneys Respond To O'Melveny-Myers ReportwtopwebAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- BB EnglishDocumento3 páginasBB EnglishwtopwebAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Landini MenuDocumento2 páginasLandini MenuwtopwebAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Whistleblower Complaint Against President TrumpDocumento9 páginasWhistleblower Complaint Against President TrumpYahoo News90% (84)
- Chesapeake Bay Crossing StudyDocumento4 páginasChesapeake Bay Crossing StudywtopwebAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Arthur Capper Senior Apartments Fire LawsuitDocumento28 páginasArthur Capper Senior Apartments Fire LawsuitwtopwebAinda não há avaliações
- Coal Roasted CarrotsDocumento2 páginasCoal Roasted CarrotswtopwebAinda não há avaliações
- D C Jail Report 2 28 19Documento39 páginasD C Jail Report 2 28 19wtopweb100% (1)
- Katerina Impact StatementDocumento7 páginasKaterina Impact StatementwtopwebAinda não há avaliações
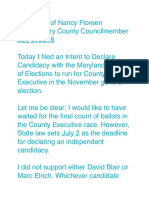
- Statement of Nancy FloreenDocumento2 páginasStatement of Nancy FloreenwtopwebAinda não há avaliações
- Cabanatuan Deaths DCDocumento12 páginasCabanatuan Deaths DCwtopweb0% (1)
- Occidental's Depression-Era Vinegar PieDocumento1 páginaOccidental's Depression-Era Vinegar PiewtopwebAinda não há avaliações
- Evidence: Daron Wint's Phone SearchesDocumento19 páginasEvidence: Daron Wint's Phone SearcheswtopwebAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Senate Statehood BillDocumento4 páginasSenate Statehood BillwtopwebAinda não há avaliações
- 2016 Election Final Report 06-14-18Documento568 páginas2016 Election Final Report 06-14-18Anonymous FBZLGrAinda não há avaliações
- Tavon Jones EssayDocumento1 páginaTavon Jones EssaywtopwebAinda não há avaliações
- Addressing Diversity Through The Years Special and Inclusive EducationDocumento3 páginasAddressing Diversity Through The Years Special and Inclusive EducationReymark Alciso EspinozaAinda não há avaliações
- Thesis Statement Disability Nancy MairsDocumento6 páginasThesis Statement Disability Nancy Mairsjaclyncreedonannarbor100% (2)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Bosh Rule 1050 Q ADocumento4 páginasBosh Rule 1050 Q ALyka GarceraAinda não há avaliações
- The Future of Disability in AmericaDocumento619 páginasThe Future of Disability in AmericaNicsparksAinda não há avaliações
- CancerWorkYou NSW LoDocumento60 páginasCancerWorkYou NSW LoAlex PiecesAinda não há avaliações
- Rethinking and Updating Demographic Questions Guidance To Improve Descriptions of Research Samples PDFDocumento15 páginasRethinking and Updating Demographic Questions Guidance To Improve Descriptions of Research Samples PDFRafael Oliveira LeiteAinda não há avaliações
- Parents Basis of Interventions To Their Child With Special NeedsDocumento28 páginasParents Basis of Interventions To Their Child With Special NeedsJenefer TionganAinda não há avaliações
- Website ReferencesDocumento3 páginasWebsite Referencesapi-356298731Ainda não há avaliações
- Edwards Syndrome: TRISOMY 18 Also Known As Trisomy E orDocumento17 páginasEdwards Syndrome: TRISOMY 18 Also Known As Trisomy E orHannahKarizaAinda não há avaliações
- Barcombe School ProspectusDocumento16 páginasBarcombe School ProspectusmrcobbsclassAinda não há avaliações
- Classroom Activity CHCDIS003Documento4 páginasClassroom Activity CHCDIS003Sonam GurungAinda não há avaliações
- Teaching Strategies and Functional Skills of Learners With Special Educational NeedsDocumento34 páginasTeaching Strategies and Functional Skills of Learners With Special Educational NeedsEditor IJTSRDAinda não há avaliações
- List of Counseling TopicsDocumento2 páginasList of Counseling TopicsDragana Modesty100% (1)
- Spangenberg Uber LawsuitDocumento60 páginasSpangenberg Uber Lawsuitmashablescribd100% (1)
- Registration Form (MIS 03-01) For T2MIS Ver.5 (3!02!18)Documento2 páginasRegistration Form (MIS 03-01) For T2MIS Ver.5 (3!02!18)Ferdinand RamaAinda não há avaliações
- Strange Geography of Health Inequalities - Susan J. Smith and Donna Easterlow, The - UnknownDocumento19 páginasStrange Geography of Health Inequalities - Susan J. Smith and Donna Easterlow, The - Unknownaaron_s_projAinda não há avaliações
- Module 12Documento4 páginasModule 12Angelica MadronaAinda não há avaliações
- PGN July 12-18, 2019Documento32 páginasPGN July 12-18, 2019Philly Gay NewsAinda não há avaliações
- Physically ChallengedDocumento8 páginasPhysically ChallengedUday Kumar100% (3)
- CWSN: State Agencies Role and Their Assistance in CWSNDocumento4 páginasCWSN: State Agencies Role and Their Assistance in CWSNApos75% (4)
- Sen Categories Chart 2022 - KeyDocumento8 páginasSen Categories Chart 2022 - KeyИрина КривоносAinda não há avaliações
- DepEd Sustains Support For Culture Based Education For IP LearnersDocumento36 páginasDepEd Sustains Support For Culture Based Education For IP LearnersKen AcevedaAinda não há avaliações
- Human Exceptionality School Community and Family 11th Edition Hardman Solutions ManualDocumento11 páginasHuman Exceptionality School Community and Family 11th Edition Hardman Solutions Manualantheagian4p4y4100% (34)
- Facilitating-Learning Book PDFDocumento337 páginasFacilitating-Learning Book PDFMichelle ArregLado VistalAinda não há avaliações
- Disability, Its Issues and Challenges: Psychosocial and Legal Aspects in Indian ScenarioDocumento11 páginasDisability, Its Issues and Challenges: Psychosocial and Legal Aspects in Indian ScenarioMHRM NIRMALAAinda não há avaliações
- Unit-3 Children and Ece ProfessionalDocumento19 páginasUnit-3 Children and Ece ProfessionalSrividya KrishnaAinda não há avaliações
- Post Graduate Diploma in Developmental Therapy: (Multiple Disabilities: Physical & Neurological)Documento29 páginasPost Graduate Diploma in Developmental Therapy: (Multiple Disabilities: Physical & Neurological)H SHABANAAinda não há avaliações
- Test Bank For Educating Exceptional Children 13th Edition KirkDocumento24 páginasTest Bank For Educating Exceptional Children 13th Edition KirkLuisWelchqapzb100% (45)
- DP - Physical Impairments - DoneDocumento13 páginasDP - Physical Impairments - Doneapi-284988119Ainda não há avaliações
- Inclusion Education Policy in IndonesiaDocumento6 páginasInclusion Education Policy in IndonesiaInternational Journal of Innovative Science and Research TechnologyAinda não há avaliações
- Perfect Murder, Perfect Town: The Uncensored Story of the JonBenet Murder and the Grand Jury's Search for the TruthNo EverandPerfect Murder, Perfect Town: The Uncensored Story of the JonBenet Murder and the Grand Jury's Search for the TruthNota: 3.5 de 5 estrelas3.5/5 (68)
- Blood Brother: 33 Reasons My Brother Scott Peterson Is GuiltyNo EverandBlood Brother: 33 Reasons My Brother Scott Peterson Is GuiltyNota: 3 de 5 estrelas3/5 (57)
- Relentless Pursuit: A True Story of Family, Murder, and the Prosecutor Who Wouldn't QuitNo EverandRelentless Pursuit: A True Story of Family, Murder, and the Prosecutor Who Wouldn't QuitNota: 4.5 de 5 estrelas4.5/5 (7)
- Our Little Secret: The True Story of a Teenage Killer and the Silence of a Small New England TownNo EverandOur Little Secret: The True Story of a Teenage Killer and the Silence of a Small New England TownNota: 4.5 de 5 estrelas4.5/5 (86)
- Altamont: The Rolling Stones, the Hells Angels, and the Inside Story of Rock's Darkest DayNo EverandAltamont: The Rolling Stones, the Hells Angels, and the Inside Story of Rock's Darkest DayNota: 4 de 5 estrelas4/5 (25)
- Killing Season: The Unsolved Case of New England's Deadliest Serial KillerNo EverandKilling Season: The Unsolved Case of New England's Deadliest Serial KillerNota: 4 de 5 estrelas4/5 (46)