Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- 7-Steps For DI Systematic ApproachDocumento8 páginas7-Steps For DI Systematic ApproachDrDeepak Pawar71% (7)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Family Therapy History Theory and Practice 6th Edition Gladding Test BankDocumento18 páginasFamily Therapy History Theory and Practice 6th Edition Gladding Test BankEdwardCarterqbfze100% (18)
- 3rd Quarter Examination in Hope 4Documento5 páginas3rd Quarter Examination in Hope 4Hazel Joan Tan100% (3)
- Tables and GraphsDocumento17 páginasTables and GraphsDrDeepak PawarAinda não há avaliações
- Data Collection FormDocumento2 páginasData Collection FormDrDeepak PawarAinda não há avaliações
- 17oncology1 Growth Disturbances TextsDocumento28 páginas17oncology1 Growth Disturbances TextsDrDeepak PawarAinda não há avaliações
- Review LiteratureDocumento23 páginasReview LiteratureDrDeepak Pawar50% (4)
- Methodology DMDocumento3 páginasMethodology DMDrDeepak PawarAinda não há avaliações
- Results and DiscussionDocumento5 páginasResults and DiscussionDrDeepak PawarAinda não há avaliações
- List of FiguresDocumento2 páginasList of FiguresDrDeepak PawarAinda não há avaliações
- Chapter 3 Aim and ObjectivesDocumento1 páginaChapter 3 Aim and ObjectivesDrDeepak PawarAinda não há avaliações
- 01 M039 43754Documento16 páginas01 M039 43754DrDeepak PawarAinda não há avaliações
- List of FiguresDocumento2 páginasList of FiguresDrDeepak PawarAinda não há avaliações
- BibliographyDocumento7 páginasBibliographyDrDeepak PawarAinda não há avaliações
- DM Conclusion 222Documento2 páginasDM Conclusion 222DrDeepak PawarAinda não há avaliações
- INTRODUCTIONDocumento5 páginasINTRODUCTIONDrDeepak PawarAinda não há avaliações
- ACRONYMSDocumento2 páginasACRONYMSDrDeepak PawarAinda não há avaliações
- Antibiotics For Upper Respiratory Tract Infections: Follow-Up Utilization and Antibiotic UseDocumento5 páginasAntibiotics For Upper Respiratory Tract Infections: Follow-Up Utilization and Antibiotic UseDrDeepak PawarAinda não há avaliações
- Oligo Research Article PDFDocumento4 páginasOligo Research Article PDFDrDeepak PawarAinda não há avaliações
- Toxicology - GeneralDocumento40 páginasToxicology - GeneralFauzan FasnidAinda não há avaliações
- 10 2 33 PDFDocumento4 páginas10 2 33 PDFDrDeepak PawarAinda não há avaliações
- Typhoid Fever AND Paratyphoid Fever: Guoli Lin Department of Infectious Diseases The Third Affiliated Hospital of SYSUDocumento70 páginasTyphoid Fever AND Paratyphoid Fever: Guoli Lin Department of Infectious Diseases The Third Affiliated Hospital of SYSUDrDeepak PawarAinda não há avaliações
- Lower Resp TRCT InfectionsDocumento45 páginasLower Resp TRCT InfectionsDrDeepak PawarAinda não há avaliações
- Barbiturate PoisoningDocumento3 páginasBarbiturate PoisoningDrDeepak PawarAinda não há avaliações
- A Seminar On Lower Respiratory Tract Infections: Click To Edit Master Subtitle StyleDocumento44 páginasA Seminar On Lower Respiratory Tract Infections: Click To Edit Master Subtitle StyleDrDeepak PawarAinda não há avaliações
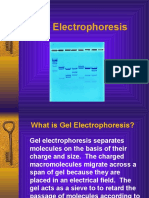
- GelelctroDocumento11 páginasGelelctroDrDeepak PawarAinda não há avaliações
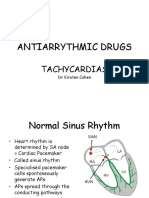
- Antiarrythmic Drugs: TachycardiasDocumento36 páginasAntiarrythmic Drugs: TachycardiasDrDeepak PawarAinda não há avaliações
- Robots in Shipbuilding Industry (1160) PDFDocumento9 páginasRobots in Shipbuilding Industry (1160) PDFWahyu WahyurachmatdhaniAinda não há avaliações
- ELECTRICAL SAFETY in The Workplace: - Ice Breaker (Mix and Match)Documento3 páginasELECTRICAL SAFETY in The Workplace: - Ice Breaker (Mix and Match)Lynn ZarAinda não há avaliações
- Hand Injuries & Their ManagementsDocumento78 páginasHand Injuries & Their ManagementsKuruAinda não há avaliações
- Method StatementDocumento20 páginasMethod StatementCharles IkenyeAinda não há avaliações
- PA1 CLASS XI P.edDocumento2 páginasPA1 CLASS XI P.edJatin GeraAinda não há avaliações
- Isabel Dela Cruz - SP Essay DraftDocumento10 páginasIsabel Dela Cruz - SP Essay Draftapi-660343728Ainda não há avaliações
- Operant ConditioningDocumento18 páginasOperant ConditioningIna GanuAinda não há avaliações
- Trends in Maternal Mortality 2000 To 2020Documento108 páginasTrends in Maternal Mortality 2000 To 2020shouka.inAinda não há avaliações
- Daftar Pustaka - 2pusssDocumento6 páginasDaftar Pustaka - 2pusssMuhammad ShodiqinAinda não há avaliações
- Health 8Documento319 páginasHealth 8Anngela Arevalo BarcenasAinda não há avaliações
- Getting Started: Normal & Slow ModesDocumento2 páginasGetting Started: Normal & Slow ModesAndy Wildan HidayatAinda não há avaliações
- Intelligent Systems and Technologies in Rehabilitation EngineeringDocumento493 páginasIntelligent Systems and Technologies in Rehabilitation EngineeringDorin Triff100% (3)
- From Bolam To Bolitho Unravelling Medical ProtectionismDocumento12 páginasFrom Bolam To Bolitho Unravelling Medical ProtectionismNatasha SieAinda não há avaliações
- Table of Specifications in Health 10Documento3 páginasTable of Specifications in Health 10Rowan ZheeAinda não há avaliações
- Edgar CayceDocumento7 páginasEdgar CayceJason MatthewsAinda não há avaliações
- Grand Strategy MatrixDocumento1 páginaGrand Strategy MatrixDominic SociaAinda não há avaliações
- MRU-QMS-HSE-Form - JSA - Geotechnical Drilling & Geotechnical Field Investigation - Rev00Documento11 páginasMRU-QMS-HSE-Form - JSA - Geotechnical Drilling & Geotechnical Field Investigation - Rev00AditAinda não há avaliações
- ScribdDocumento29 páginasScribdeshasohail789Ainda não há avaliações
- ISSLDocumento58 páginasISSLsufiAinda não há avaliações
- Liver & Biliary DiseaseDocumento41 páginasLiver & Biliary Diseasesaump3Ainda não há avaliações
- Courses - Downloads - 2019 Batch - Dual Degree CurriculumDocumento86 páginasCourses - Downloads - 2019 Batch - Dual Degree CurriculumSreejith N ch19b090Ainda não há avaliações
- Language Development: - Iphy OkoyeDocumento9 páginasLanguage Development: - Iphy OkoyeIPHY OKOYEAinda não há avaliações
- Anatomical Foundations of Chinese MedDocumento29 páginasAnatomical Foundations of Chinese Medanattā100% (1)
- Dependent Personality DisorderDocumento14 páginasDependent Personality DisorderPalak GuptaAinda não há avaliações
- Controlling Genset NoiseDocumento2 páginasControlling Genset NoiseNishant BhavsarAinda não há avaliações
- Personal Philosophy Statement Assignment 2017Documento2 páginasPersonal Philosophy Statement Assignment 2017api-538727441Ainda não há avaliações
- Microbiome and CancerDocumento63 páginasMicrobiome and CancerK C Goutham ReddyAinda não há avaliações
- Case Study PresentationDocumento19 páginasCase Study PresentationShariq Siddiqui100% (1)