Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Anapersi by IcingDocumento1 páginaAnapersi by IcingSodiqa Strida SaSi TwinzAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Tere Liye TranslateDocumento1 páginaTere Liye TranslateSodiqa Strida SaSi TwinzAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Examination Lumps and BumpsDocumento4 páginasExamination Lumps and BumpsSodiqa Strida SaSi TwinzAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Examination Lumps and BumpsDocumento4 páginasExamination Lumps and BumpsSodiqa Strida SaSi TwinzAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Hepatitis A: Questions and Answers: Information About The Disease and VaccinesDocumento4 páginasHepatitis A: Questions and Answers: Information About The Disease and VaccinesSodiqa Strida SaSi TwinzAinda não há avaliações
- Metabolic Factors in OADocumento24 páginasMetabolic Factors in OASodiqa Strida SaSi TwinzAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Annual Reports in Medicinal Chemistry Vol 40 2005 IsBN 0120405407 9780120405404 Page 9 Epilepsy Link 2005.Documento519 páginasAnnual Reports in Medicinal Chemistry Vol 40 2005 IsBN 0120405407 9780120405404 Page 9 Epilepsy Link 2005.Samantha DearnaleyAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Project 2 Nathan ChaulkDocumento17 páginasProject 2 Nathan Chaulkapi-535482465Ainda não há avaliações
- The Status and Prospects of The Licensed Pharmacist Qualification System in ChinaDocumento5 páginasThe Status and Prospects of The Licensed Pharmacist Qualification System in ChinaiisteAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Mr. Swapnil L. Patil: Presented ByDocumento66 páginasMr. Swapnil L. Patil: Presented Byaakash sahaAinda não há avaliações
- Cleaning Validation in Pharmaceutical IndustriesDocumento10 páginasCleaning Validation in Pharmaceutical Industriessamia khanAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Cefpodoxime 200 Tab New 1Documento25 páginasCefpodoxime 200 Tab New 1Gurdev SinghAinda não há avaliações
- The Junk Science Self Defense Manual by Anthony ColpoDocumento30 páginasThe Junk Science Self Defense Manual by Anthony ColpoacolpoAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
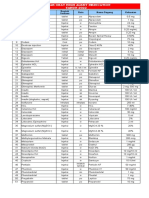
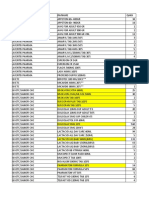
- Daftar Lasa Ham Obat Resiko JatuhDocumento4 páginasDaftar Lasa Ham Obat Resiko JatuhAbu Hisyam Al KhendaryAinda não há avaliações
- Managing Otitis ExternaDocumento34 páginasManaging Otitis ExternaramaAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Drug Classification - PhenytoinDocumento3 páginasDrug Classification - Phenytoinkedwards108Ainda não há avaliações
- White PaperDocumento40 páginasWhite PaperMohammad IsmailAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Ra 9711Documento12 páginasRa 9711Femina ArgonzaAinda não há avaliações
- F&IP Lab Manual 4th YearDocumento173 páginasF&IP Lab Manual 4th YearVargheseAinda não há avaliações
- Effect of Shatapushpa Taila Matra Basti and Pathadi Kwatha On Poly Cystic OvarianDocumento4 páginasEffect of Shatapushpa Taila Matra Basti and Pathadi Kwatha On Poly Cystic Ovarianshenali nadeesha100% (1)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- WikiLeaks Podesta Email Release Google Doc As of October 31, 2016Documento88 páginasWikiLeaks Podesta Email Release Google Doc As of October 31, 2016Joe Smith100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Oral Candidiasis - A Case ReportDocumento4 páginasOral Candidiasis - A Case ReportDevinta RubaiAinda não há avaliações
- SakajajaDocumento34 páginasSakajajavini nurbaitiAinda não há avaliações
- Validation 124Documento13 páginasValidation 124Donig FermanianAinda não há avaliações
- 1885 2Documento73 páginas1885 2JuhiJahan AmanullahAinda não há avaliações
- Mumbai ListDocumento2.744 páginasMumbai ListShuBham Is Live100% (1)
- Overview Beta BlockersDocumento11 páginasOverview Beta BlockersginafujiAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- CDDS ClassificationDocumento63 páginasCDDS ClassificationAna MacoveiAinda não há avaliações
- Chapter 01Documento21 páginasChapter 01Jan MarcusAinda não há avaliações
- Rini Hamsidi, Adryan Fristiohady, Nasyrah Musabar: Majalah Farmasi, Sains, Dan Kesehatan ISSN 2442-9791Documento4 páginasRini Hamsidi, Adryan Fristiohady, Nasyrah Musabar: Majalah Farmasi, Sains, Dan Kesehatan ISSN 2442-9791Puskesmas SambongAinda não há avaliações
- QC Test For CapsulesDocumento4 páginasQC Test For CapsulesMuhammad Masoom Akhtar100% (1)
- Paracetamol Injection Products in PakistanDocumento1 páginaParacetamol Injection Products in PakistanAltaf Ur RehmanAinda não há avaliações
- Eviyana: Fresh Graduate Education SkillsDocumento3 páginasEviyana: Fresh Graduate Education SkillseviyanaAinda não há avaliações
- Nurse-Led Clinics: Accountability and PracticeDocumento5 páginasNurse-Led Clinics: Accountability and PracticeFlor OMAinda não há avaliações
- Antimicrobial Effectiveness Test GMP InvestigationsDocumento8 páginasAntimicrobial Effectiveness Test GMP Investigationsgge2502Ainda não há avaliações
- Environmental Monitoring HandbookDocumento38 páginasEnvironmental Monitoring HandbookKraken Ur100% (3)