Você também pode gostar
- Jurnal 4Documento6 páginasJurnal 4Dea MaulidiaAinda não há avaliações
- Glaucoma - A Eye Disorder Its Causes, Risk Factor, Prevention and MedicationDocumento16 páginasGlaucoma - A Eye Disorder Its Causes, Risk Factor, Prevention and MedicationDea MaulidiaAinda não há avaliações
- 5 Surat Al MaidahDocumento101 páginas5 Surat Al MaidahDea MaulidiaAinda não há avaliações
- Ijo 24 69 PDFDocumento6 páginasIjo 24 69 PDFPutri Nisrina HamdanAinda não há avaliações
- Dinda SDocumento16 páginasDinda SLulu SupergirlAinda não há avaliações
- 466 919 1 SMDocumento4 páginas466 919 1 SMArinaBintangAfrianAinda não há avaliações
- Gestational Trophoblastic Disease GTDDocumento39 páginasGestational Trophoblastic Disease GTDDea Maulidia100% (1)
- 3 - Surat Ali ImranDocumento120 páginas3 - Surat Ali ImranAditya Arya PutraAinda não há avaliações
- Anesthesia in The District HospitalDocumento162 páginasAnesthesia in The District HospitalPrayudi Aji MurtoloAinda não há avaliações
- Gestational Trophoblastic Disease (GTD - Version Gao)Documento72 páginasGestational Trophoblastic Disease (GTD - Version Gao)Dea MaulidiaAinda não há avaliações
- Review Article Dental 2Documento6 páginasReview Article Dental 2Dea MaulidiaAinda não há avaliações
- RCCM 201111-1992edDocumento3 páginasRCCM 201111-1992edDea MaulidiaAinda não há avaliações
- Gestational Trophoblastic Disease-1Documento18 páginasGestational Trophoblastic Disease-1Dea MaulidiaAinda não há avaliações
- Journal Reading NieskaDocumento4 páginasJournal Reading NieskaDea MaulidiaAinda não há avaliações
- 2016 Monthly CalendarDocumento12 páginas2016 Monthly CalendarDea MaulidiaAinda não há avaliações
- WP097Documento16 páginasWP097Dea MaulidiaAinda não há avaliações
- RCMB 2009-0160ocDocumento7 páginasRCMB 2009-0160ocDea MaulidiaAinda não há avaliações
- Us 7680538Documento6 páginasUs 7680538Dea MaulidiaAinda não há avaliações
- RCMB 2005-0317oeDocumento6 páginasRCMB 2005-0317oeDea MaulidiaAinda não há avaliações
- Pats 200709-155mgDocumento8 páginasPats 200709-155mgDea MaulidiaAinda não há avaliações
- Pulmonary, Sleep, and Critical Care Updates: Update in Sleep Medicine 2010Documento5 páginasPulmonary, Sleep, and Critical Care Updates: Update in Sleep Medicine 2010Dea MaulidiaAinda não há avaliações
- RCCM 200412-1631soDocumento8 páginasRCCM 200412-1631soDea MaulidiaAinda não há avaliações
- Specific FractureDocumento19 páginasSpecific FractureDiaz RandanilAinda não há avaliações
- 1 s2.0 S042276381300191X MainDocumento7 páginas1 s2.0 S042276381300191X MainDea MaulidiaAinda não há avaliações
- Fracture MGT 2Documento41 páginasFracture MGT 2Ranjith CRAinda não há avaliações
- CTEVDocumento7 páginasCTEVRhiri ElbieAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5783)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- ICS Cancer Sahyog Medical Assistance FormDocumento1 páginaICS Cancer Sahyog Medical Assistance FormMd Waseem KAinda não há avaliações
- Case Study Project: Elective - Healthcare & Hospital ManagementDocumento2 páginasCase Study Project: Elective - Healthcare & Hospital ManagementlucasAinda não há avaliações
- Molecular Imaging: GE HealthcareDocumento11 páginasMolecular Imaging: GE HealthcarexibearAinda não há avaliações
- Graduate Outstanding PTsDocumento20 páginasGraduate Outstanding PTsamir alamAinda não há avaliações
- NEW m1m2 Reporting FormDocumento24 páginasNEW m1m2 Reporting FormDeyeck Verga100% (8)
- Ayushman Bharat PMJAY Branding GuidelinesDocumento10 páginasAyushman Bharat PMJAY Branding GuidelinesalkaAinda não há avaliações
- Mouth Preparation For Removable Partial DentureDocumento84 páginasMouth Preparation For Removable Partial DentureDrVarun Menon100% (2)
- PDF 2420872588Documento1 páginaPDF 2420872588kariem noweerAinda não há avaliações
- Doctor Mahavir EnclaveDocumento22 páginasDoctor Mahavir EnclaveFortune BuildersAinda não há avaliações
- Nursing Management - Concepts and Principles of ManagementDocumento4 páginasNursing Management - Concepts and Principles of Managementsoundaramilangovan254989% (9)
- Philosophy of Nursing Service in HospitalDocumento11 páginasPhilosophy of Nursing Service in HospitalAprille Sgrr100% (4)
- About Rectal TubeDocumento3 páginasAbout Rectal TubeElpanUmbalanAinda não há avaliações
- Health Information Exchange Fact SheetDocumento4 páginasHealth Information Exchange Fact SheetDavid MarkAinda não há avaliações
- Daftar PustakaDocumento4 páginasDaftar PustakaNadya Allencia WijayaAinda não há avaliações
- Client Satisfaction and Quality of Health Care in Rural BangladeshDocumento6 páginasClient Satisfaction and Quality of Health Care in Rural BangladeshMizanur RahmanAinda não há avaliações
- Module 01: Overview of Public Health Nursing in The PhilippinesDocumento6 páginasModule 01: Overview of Public Health Nursing in The PhilippinesHazelAinda não há avaliações
- Public-Notice-Telemedicine-Practice-Guidelines MKKNJ NnjiDocumento33 páginasPublic-Notice-Telemedicine-Practice-Guidelines MKKNJ NnjiNIHUGBH KOLKATAAinda não há avaliações
- Blockchain in Healthcare: Guangjian Huang, Abdullah Al FoysalDocumento14 páginasBlockchain in Healthcare: Guangjian Huang, Abdullah Al Foysalshubham thkAinda não há avaliações
- Comparison of Services Between Public and Private HospitalsDocumento10 páginasComparison of Services Between Public and Private HospitalsJahidul IslamAinda não há avaliações
- InterpreterDocumento12 páginasInterpreterXinyue XuAinda não há avaliações
- Residency Survival Guide: Canadian Association of General Surgeons Residents CommitteeDocumento53 páginasResidency Survival Guide: Canadian Association of General Surgeons Residents CommitteeIrina MincuAinda não há avaliações
- Acing The Orthopedic Board ExamDocumento481 páginasAcing The Orthopedic Board ExamMark M. Alipio100% (9)
- Test Bank For Essentials of Dental Assisting 6th Edition by RobinsonDocumento8 páginasTest Bank For Essentials of Dental Assisting 6th Edition by Robinsonashleyhaaswxcbmagsde100% (30)
- National Curriculum Framework ReviewDocumento16 páginasNational Curriculum Framework ReviewSuryaAinda não há avaliações
- Week 2: Post-Marketing Regulation of Pharmaceutical Products LearningDocumento4 páginasWeek 2: Post-Marketing Regulation of Pharmaceutical Products LearningNics PedrezuelaAinda não há avaliações
- Uganda Health Sector and Partnership Opportunities Final PDFDocumento69 páginasUganda Health Sector and Partnership Opportunities Final PDFPatrickLnanduAinda não há avaliações
- Auckland DHB Annual Report 2012/2013 HighlightsDocumento108 páginasAuckland DHB Annual Report 2012/2013 HighlightsGeorge BanksAinda não há avaliações
- Journal Reading Kelompok 3 Periode 13 April-6 Mei 2020-DikonversiDocumento37 páginasJournal Reading Kelompok 3 Periode 13 April-6 Mei 2020-DikonversiIKM FKUNSOEDAinda não há avaliações
- PPD Pertemuan 12 (Klasifikasi Tes Psikologi HIMPSI)Documento32 páginasPPD Pertemuan 12 (Klasifikasi Tes Psikologi HIMPSI)Pengisi Dompet50% (2)
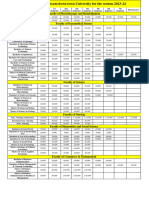
- Fees Structure Assam Down Town University For The Session 2023 2Documento2 páginasFees Structure Assam Down Town University For The Session 2023 2Debashish SharmaAinda não há avaliações