Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Anabolic Peptide Beta EbookDocumento226 páginasAnabolic Peptide Beta EbookMatei Cipri80% (5)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Gallstone e BookDocumento107 páginasGallstone e Bookee1993Ainda não há avaliações
- ATI Ebook - Med SurgDocumento702 páginasATI Ebook - Med SurgMichelle Villanueva100% (4)
- OSCES Mock Marking SchemeDocumento126 páginasOSCES Mock Marking SchemeJennifer MotwaniAinda não há avaliações
- Pathology Mci One Liners MCQDocumento21 páginasPathology Mci One Liners MCQadiAinda não há avaliações
- Role of Critical Care Nurses in End-of-Life CareDocumento32 páginasRole of Critical Care Nurses in End-of-Life Carejohn christopher JimenezAinda não há avaliações
- ACLS AlgorithmsDocumento4 páginasACLS Algorithmsmonickams100% (1)
- CVS PDFDocumento102 páginasCVS PDFmalik003Ainda não há avaliações
- Label Nama Obat Di Rak ObatDocumento6 páginasLabel Nama Obat Di Rak Obatanon_756054910Ainda não há avaliações
- Cranial Nerve AssessmentDocumento42 páginasCranial Nerve Assessmentmalik003100% (1)
- Dha Exam..Muhammad IbrahimDocumento11 páginasDha Exam..Muhammad Ibrahimmalik003100% (4)
- Lecture 1 History of SurgeryDocumento7 páginasLecture 1 History of SurgeryRosa PalconitAinda não há avaliações
- Recent Advances in The Development of Anti-Tuberculosis Drugs Acting On Multidrug-Resistant Strains: A ReviewDocumento18 páginasRecent Advances in The Development of Anti-Tuberculosis Drugs Acting On Multidrug-Resistant Strains: A Reviewmalik003Ainda não há avaliações
- Challan FormDocumento1 páginaChallan FormFurqan ButtAinda não há avaliações
- VascularDisordersLiver2009 PDFDocumento36 páginasVascularDisordersLiver2009 PDFmalik003Ainda não há avaliações
- Visa Sopporting Documents Attach List: Dr. Zaheer Ahmed, MBBSDocumento1 páginaVisa Sopporting Documents Attach List: Dr. Zaheer Ahmed, MBBSmalik003Ainda não há avaliações
- SummariesDocumento140 páginasSummariesmalik003Ainda não há avaliações
- Usmle Cs NotesDocumento16 páginasUsmle Cs NotesJason Steel100% (1)
- Career Opportunities For MBBS Doctors On Contract Basis Udate 21-2-2017Documento2 páginasCareer Opportunities For MBBS Doctors On Contract Basis Udate 21-2-2017malik003Ainda não há avaliações
- RLDocumento1 páginaRLmalik003Ainda não há avaliações
- History in Ob/Gy: Ahmed AbdulwahabDocumento9 páginasHistory in Ob/Gy: Ahmed Abdulwahabmalik003Ainda não há avaliações
- Bleeding Disorder ApproachDocumento9 páginasBleeding Disorder Approachmalik003Ainda não há avaliações
- Gs Instruments 121029054516 Phpapp01Documento87 páginasGs Instruments 121029054516 Phpapp01malik003Ainda não há avaliações
- 6868841Documento35 páginas6868841malik003Ainda não há avaliações
- CR Oh Ns Disease in Adults 2009Documento19 páginasCR Oh Ns Disease in Adults 2009ostosjesus4824Ainda não há avaliações
- Recommendations for Testing, Managing, and Treating Hepatitis CDocumento12 páginasRecommendations for Testing, Managing, and Treating Hepatitis Cmalik003Ainda não há avaliações
- Unilateral Enlarged Kidney PDFDocumento2 páginasUnilateral Enlarged Kidney PDFmalik003Ainda não há avaliações
- Recommendations For Testing, Managing, and Treating Hepatitis C - MANAGEMENT of ACUTE HCV INFECTION - 2015-06-29Documento8 páginasRecommendations For Testing, Managing, and Treating Hepatitis C - MANAGEMENT of ACUTE HCV INFECTION - 2015-06-29malik003Ainda não há avaliações
- Cranialnerveexamination 111106073102 Phpapp02Documento49 páginasCranialnerveexamination 111106073102 Phpapp02Suleiman AbdallahAinda não há avaliações
- HSE-CPSP Postgraduate Scholarship Programme: 2 Year Exchange Training Programme in IrelandDocumento23 páginasHSE-CPSP Postgraduate Scholarship Programme: 2 Year Exchange Training Programme in IrelandDrShoaib SaadatAinda não há avaliações
- DHA Paper 17.12.15 DR - Sadaf AyazDocumento5 páginasDHA Paper 17.12.15 DR - Sadaf Ayazmalik003Ainda não há avaliações
- 6868841Documento35 páginas6868841malik003Ainda não há avaliações
- Advertisement and Job Application Form For Various Posts at Punjab Health Facilities Management Company (17.07.2017)Documento8 páginasAdvertisement and Job Application Form For Various Posts at Punjab Health Facilities Management Company (17.07.2017)HooriaKhanAinda não há avaliações
- April 24: Zein Mahgoub PACES Simplified Zein MahgoubDocumento4 páginasApril 24: Zein Mahgoub PACES Simplified Zein Mahgoubmalik003Ainda não há avaliações
- Prosthetic Valve PDFDocumento3 páginasProsthetic Valve PDFmalik003Ainda não há avaliações
- Urgent Required Female Staff NursesDocumento1 páginaUrgent Required Female Staff Nursesmalik003Ainda não há avaliações
- Prevention of Venous Thromboembolism in Nonsurgical PatientsDocumento23 páginasPrevention of Venous Thromboembolism in Nonsurgical Patientsmalik003Ainda não há avaliações
- GR 080013Documento3 páginasGR 080013malik003Ainda não há avaliações
- 6868841Documento35 páginas6868841malik003Ainda não há avaliações
- Drug-induced rheumatic syndromes: the need to be awareDocumento2 páginasDrug-induced rheumatic syndromes: the need to be awaredentsavvyAinda não há avaliações
- Pathophysiology and Treatment of SevereDocumento13 páginasPathophysiology and Treatment of SevereIva Pinasti DestaraniAinda não há avaliações
- "Physiological Monitoring and Device Interface": Report by Jawia Mustapha BSN2-ADocumento21 páginas"Physiological Monitoring and Device Interface": Report by Jawia Mustapha BSN2-ADimple AnticamaraAinda não há avaliações
- ADENOMYOSISDocumento5 páginasADENOMYOSISdoddydrAinda não há avaliações
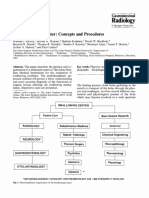
- 4.3 Swallowing - Center - Concepts - and - ProceduresDocumento7 páginas4.3 Swallowing - Center - Concepts - and - Proceduresluribe662Ainda não há avaliações
- Radiographer Job SpecDocumento5 páginasRadiographer Job SpecSherbet Spence0% (1)
- Urology Case Reports: Daniel Ensley, Grant H. EvansDocumento2 páginasUrology Case Reports: Daniel Ensley, Grant H. EvansFrankenstein MelancholyAinda não há avaliações
- Acupuncture For Children With Autism Spectrum Disorders - A Systematic Review of Randomized Clinical TrialsDocumento14 páginasAcupuncture For Children With Autism Spectrum Disorders - A Systematic Review of Randomized Clinical TrialsPaul NguyenAinda não há avaliações
- Organization Structure and Functioning of Garden City CollegeDocumento62 páginasOrganization Structure and Functioning of Garden City CollegeManilalPAinda não há avaliações
- Pediatric Emergency SDL Case Discussion Group 3Documento14 páginasPediatric Emergency SDL Case Discussion Group 3Russell Talan CilotAinda não há avaliações
- Stab WoundsDocumento57 páginasStab WoundsMushtaq AhmadAinda não há avaliações
- Cancer IntroDocumento29 páginasCancer Intromara5140Ainda não há avaliações
- Final NPRD, 2021Documento28 páginasFinal NPRD, 2021Maruthi RoshanAinda não há avaliações
- September 2011Documento38 páginasSeptember 2011Ricardo Huchiyama TakayamaAinda não há avaliações
- Laporan UgdDocumento32 páginasLaporan UgdGizi Manis JayaAinda não há avaliações
- SOP: Injections in Dogs and CatsDocumento4 páginasSOP: Injections in Dogs and CatsClaritha TaopanAinda não há avaliações
- Diabetic Retinopathy Treatment in MumbaiDocumento7 páginasDiabetic Retinopathy Treatment in MumbaiCharvi JainAinda não há avaliações
- Melioidosis.: Burkholderia PseudomalleiDocumento34 páginasMelioidosis.: Burkholderia Pseudomalleitummalapalli venkateswara raoAinda não há avaliações
- 1 SM PDFDocumento7 páginas1 SM PDFFarhatun Qolbiyah YayaAinda não há avaliações
- Introduction To Pharmacy Lecture Notes - Doc LanchaDocumento36 páginasIntroduction To Pharmacy Lecture Notes - Doc LanchaMignot Ayenew100% (1)
- Shingles RecombinantDocumento2 páginasShingles Recombinantn99aliAinda não há avaliações