Open Science Journal of Clinical Medicine
2014; 2(1): 39-43
Published online February 28, 2014 (http://www.openscienceonline.com/journal/osjcm)
Hypertensive heart failure in Kumasi, Ghana
Isaac Kofi Owusu1, 2, Yaw Adu-Boakye2, Lambert Appiah Tetteh2
1
2
Department of Medicine, College of Health Sciences, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana
Department of Medicine, Komfo Anokye Teaching Hospital, Kumasi, Ghana
Email address
ikeowusu@yahoo.com (I. K. Owusu)
To cite this article
Isaac Kofi Owusu, Yaw Adu-Boakye, Lambert Appiah Tetteh. Hypertensive Heart Failure in Kumasi, Ghana, Open Science Journal of
Clinical Medicine. Vol. 2, No. 1, 2014, pp. 39-43
Abstract
Hypertension has become a major public health issue worldwide, and it has been found to be the most common cause of
heart failure in many parts of sub-Saharan Africa. This was an observational study designed to determine the
demographic and clinical characteristics of hypertensive heart failure patients seen at the department of medicine, Komfo
Anokye Teaching Hospital (KATH), Kumasi, Ghana. Medical records of 180 hypertensive heart failure patients were
selected using simple random sampling. The baseline demographic, clinical, chest X-ray, electrocardiographic (ECG)
and echocardiographic characteristics of the patients were examined. One hundred and eighty (180) hypertensive heart
failure were studied. They were aged between 24 - 88 years with the mean age ( SD) of 63.59 (18.12) years. There
were more females (52.22%; n=94) than males (47.78%; n=86). The mean systolic blood pressure ( SD) and the mean
diastolic blood pressure ( SD) were 162.42 ( 32.18) and 92.29 (18.54) respectively. The pulse rate ranged between
43-168 beats/minute with the mean pulse rate ( SD) of 85.24 ( 20.71) beats/minute. Most (46 %) of the patients
presented with NYHA functional class 4. The most common presenting complaint was shortness of breath (72.22%),
followed by easy fatiguability (50%), and palpitation (43.89%). The main clinical signs were pulmonary oedema (80%)
and displaced apex beat (67.78%). Chest X-ray showed cardiomegaly in 71.11% of the patients. ECG LVH and
echocardiographic LVH were seen in 75.56 % and 83.33% of the patients respectively. Prevalence of heart failure with
preserve ejection fraction (HFPEF) was 62.22 %. Left ventricular systolic dysfunction with or with diastolic dysfunction
was seen in 37.78 % of the patients. In conclusion, the most common clinical presentation of patients seen at KATH,
Kumasi, with hypertensive heart failure were shortness of breath, easy fatiguability, pulmonary oedema and displaced
apex beat. The prevalence of heart failure with preserved ejection fraction (HFPEF) among the patients was high.
Keywords
Hypertension, Heart Failure, Prevalence, Left Ventricular Hypertrophy, Ghana
1. Introduction
Hypertension has become a major public health issue
worldwide. In sub-Saharan Africa, morbidity and mortality
of hypertensive related conditions has reached epidemic
levels in recent years. [1-4]. It has been estimated that
hypertension associated morbidity in sub-Saharan Africa
may rise to 20% by the year 2020 [5].
Hypertension is the most common cause of heart failure
in many parts of sub-Saharan Africa [4, 6-10], and
hypertension has been reported to account for up to 30 %
of hospital admissions for heart failure in West Africa [11].
Hypertension is also a powerful independent risk factor for
death from heart disease [12]. The prognosis of
hypertensive heart failure among Black Africans has also
been found to be poor [13].
There is evidence from large population-based studies of
an increased tendency to left ventricular hypertrophy in
hypertensive blacks, independent of body composition [14].
Hypertension may also result in interstitial fibrosis [15].
Both factors contribute to an increase in left ventricle
stiffness, resulting in diastolic dysfunction and an elevation
40
Isaac Kofi Owusu et al.: Hypertensive Heart Failure in Kumasi, Ghana
in left ventricular end diastolic pressure.
Left ventricular hypertrophy is not an acute condition. It
takes weeks and usually months to years to develop. It has
been proposed that a cardiac renin-angiotensin system and
angiotensin converting enzyme activity may be an
important determinant of the hypertrophic response [16].
There are two predominant types of hypertrophy:
concentric; where wall thickness is increased relative to
cavity dimensions, and eccentric; where there is left
ventricular cavity dilatation, with an increase in muscle
mass so that the ratio between wall thickness and
ventricular cavity size remains relatively constant.
Three types of hypertensive heart failure (types I-III)
have been described [16]. In type I hypertensive heart
failure, the decompensated myocardium is still strong
enough to sustain a high blood pressure and patients with
this type present with high blood pressure on admission.
Patients with type II hypertensive heart failure may present
with a low or normal blood pressure initially; following
treatment of the heart failure, the decompensated
myocardium may recover sufficiently enough for the blood
pressure to rise again few days after the commencement of
treatment. In type III hypertensive heart failure, the
decompensated myocardium has been irreversibly
damaged by the chronic uncontrolled hypertension that
despite adequate treatment of the heart failure, the
myocardium is not strong enough to sustain a high blood
pressure any longer [17]. The types II and III can easily be
mistaken for cardiomyopathy.
The aim of this study was to determine the demographic
and clinical characteristics of hypertensive heart failure
patients seen at the department of medicine, KATH,
Kumasi.
Hypertension was defined as the presence of a persistent
elevated systolic blood pressure 140mmHg and/or
diastolic blood pressure 90mmHg in patients aged 15
years and above [19, 20], and/or presence of hypertensive
retinopathy and/or the use of antihypertensive drugs and/or
past medical history of hypertension.
All the study participants had standard trans-thoracic
echocardiographic procedures performed by the author.
The echocardiographic data of the patients which were
obtained included; m-mode, 2- dimensional, doppler,
colour flow imaging, and valvular apparatus characteristics.
Left ventricular systolic dysfunction was defined as left
ventricular ejection fraction (EF) < 50%. Heart failure with
preserve ejection fraction (HFPEF) was defined as isolated
diastolic dysfunction (EF > 50%). Left ventricular diastolic
dysfunction was defined as E/A ratio<1 or E/A ratio >2,
DT>220ms or DT<160ms, IVRT>100ms or IVRT < 70ms.
Tissue Doppler imaging could not be done.
Resting 12-lead ECGs were obtained from 180 of the
hypertensive heart failure patients. The ECGs were
examined for the heart rate, the rhythm, electrical
conduction, chamber enlargement, arrhythmias, and other
abnormalities. Left ventricular hypertrophy was diagnosed
using Scott's criteria [21]
2. Materials and Methods
3. Statistical Analysis
This was a descriptive study carried out at the
Department of Medicine of Komfo Anokye Teaching
Hospital (KATH), Kumasi, Ghana. Ethical approval was
obtained from the appropriate ethical committee.
Medical records of 180 hypertensive heart failure
patients were selected using simple random sampling. The
baseline
demographic,
clinical,
chest
X-ray,
electrocardiographic and echocardiographic characteristics
of the patients were examined.
Heart failure was
diagnosed, using the modified Framingham criteria for the
diagnosis of heart failure [7, 8, 18]:
Major criteria included: Paroxysmal nocturnal dyspnoea,
raised jugular venous pressure, clinical cardiomegaly, basal
crepitations, S3 gallop, clinical acute pulmonary oedema,
pulmonary upper lobe blood diversion on chest X-ray (or
pulmonary oedema on chest X-ray).
Minor criteria included: tachycardia, orthopnoea,
exertional dyspnoea, nocturnal cough, hepatomegaly,
pleural effusion, diuretic use.
Heart failure was diagnosed if the patient had two major
and one minor or one major and two minor criteria
Data from the patients medical records were entered
into a Microsoft Excel (2010) sheet. Data were cleaned and
abnormal variable and wrong entry removed or changed.
Data were then exported into SPSS 16.0 software for
analysis. Descriptive analysis of baseline parameters was
provided. Measure of central tendency using mean was
calculated, and measure of spread using standard deviation
and range were also calculated.
4. Results
One hundred and eighty (180) hypertensive heart failure
patients were studied. They were aged between 24 - 88
years with the mean age ( SD) of 63.59 (18.12) years.
There were more females (52.22%; n=94) than males
(47.78%; n=86). The mean age ( SD) of the females and
the males were 64.52 (18.84) and 62.57 (17.33)
respectively. The mean systolic blood pressure ( SD) and
the mean diastolic blood pressure ( SD) were 162.42 (
32.18) and 92.29 (18.54) respectively. The pulse rate
ranged between 43-168 beats/minute with the mean pulse
Open Science Journal of Clinical Medicine 2014, 2(1): 39-43
41
rate ( SD) of 85.24 ( 20.71) beats/minute. Table 1 shows
baseline characteristics of the hypertensive heart failure
patients.
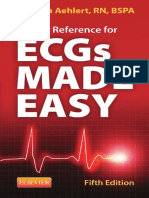
Figure 1 shows the New York Heart Association (NYHA)
functional classification of the patients. Most (46 %) of the
patients presented with NYHA functional class 4, followed
by NYHA functional class 3 (34%).
Table 2. showing the clinical presentation of the hypertensive heart failure
patients.
Table 1. showing the baseline characteristics of the hypertensive heart
failure patients.
Shortness of breath
130
72.22
Easy fatiguability
90
50
Palpitation
79
43.89
Cough
62
34.44
Chest pain
34
18.89
Pulmonary oedema
144
80
Displaced apex beat
122
67.78
Systemic oedema
81
45
Chest X-ray cardiomegaly
128
71.11
ECG LVH
136
75.56
Echocardiographic LVH
150
83.33
HFPEF
112
62.22
24-86 years
LVSD ( diastolic dysfunction)
68
37.78
30-88 years
HFPEF=heart failure with preserve ejection fraction, LVSD=left
ventricular systolic dysfunction
ECG=electrocardiographic, LVH=left ventricular hypertrophy
Baseline
Characteristics
Mean (SD)
Range
Age
63.59 (18.12)
24-88 years
Systolic Blood
Pressure (SBP)
162.42 (32.18)
126-250 mmHg
Clinical Presentation
Symptoms
Signs
Other characteristics
Diastolic Blood
Pressure (DBP)
92.29 (18.54)
56-160 mmHg
Pulse Rate
85.24 ( 20.71)
43-168 beats/minute
Male (47.78%; n=86)
Age
62.57 (17.33)
Females (52.22%; n=94)
Age
64.52 (18.84)
5. Discussion
Figure 1. showing the New York Heart Association Functional
Classification of the patients.
Table 2 shows the clinical presentation of the patients.
The most common presenting complaint was shortness of
breath (72.22%), followed by easy fatiguability (50%), and
palpitation (43.89%). The main clinical signs were
pulmonary oedema (80%) and displaced apex beat
(67.78%). Chest X-ray showed cardiomegaly in 71.11% of
the patients. ECG LVH and Echocardiographic LVH were
seen in 75.56 % and 83.33% of the patients respectively.
Prevalence of heart failure with preserve ejection fraction
(HFPEF) was 62.22 %. Left ventricular systolic
dysfunction with or with diastolic dysfunction was seen in
37.78 % of the patients.
The mean age ( SD) of the patients in this study was
63.59 (18.12). The mean age was slightly higher than the
mean age of patients with heart failure reported by earlier
studies in Kumasi [6, 8, 22], Accra [7] and other parts of
West Africa [23]. Isezuo et al [23] reported that the mean
age of Gambians and Nigerians with heart failure was 53
( 12.1). However, Oyoo and Ogola in Nairobi, Kenya
found three quarters of their patients with hypertensive
heart failure to be above the age of 50 years [24]. An
earlier study in Kumasi, Ghana among hypertensive heart
failure patients found a median age of 60 years [25]. In
sub-Saharan Africa, other important causes of heart failure
such as rheumatic heart disease and dilated
cardiomyopathy occur at a relatively early age whilst
hypertensive heart disease occurs at a later age. This might
explain the higher mean age for patients presenting with
hypertensive heart failure as compared to the mean age of
patients presenting with heart failure in sub-Saharan Africa.
The mean age of patients presenting with heart failure in
sub-Saharan Africa is generally lower than the mean age
heart failure patients reported in the general European
population (74 years) and in the Framingham heart study
(70 10.8 years) [26, 27]. Thus, heart failure occurs a
decade earlier in sub-Saharan Africa than in Europe and
America. Besides differences in aetiology of heart failure
in sub-Saharan Africa and the Western world, many people
with myocardial infarction in Europe and America are
surviving because of advances in treatment, and these
42
Isaac Kofi Owusu et al.: Hypertensive Heart Failure in Kumasi, Ghana
patients eventually end up with heart failure later in life.
The severity of heart failure at presentation using the
NYHA functional classification in this study is similar to
the findings of Oyoo and Ogola in Nairobi where majority
of their patients were in NYHA functional class IV [24].
This finding shows that many patients with heart failure in
sub-Saharan Africa present to the hospital late. This is
unfortunate because patients with asymptomatic heart
failure are more likely to achieve reverse cardiac
remodeling and normal cardiac function when neurohormonal blocking agents are started early.
The mean SBP (162.42 32.18 mmHg) and the mean
DBP (92.29 18.54 mmHg) of the patients in this study
were high. An earlier study in Kumasi also reported high
mean SBP and mean DBP of 175 15 mmHg and 112 24
mmHg respectively [25]. Isezuo et al [23] reported high
mean SBP and mean DBP of 180.4 28.2 mmHg and 117
12.9 mmHg respectively, among Gambians and
Nigerians with hypertensive heart failure. Another study in
Nigeria found the mean SBP and the mean DBP as 167.4
18.2 mmHg and 98.6 13.5 mmHg respectively [28].
Studies have demonstrated that as the SBP and the DBP
increase, the risk of cardiovascular events increases
continuously [29]. A positive relationship between diastolic
dysfunction and the level of the BP has also been
established [30], with the degree of the diastolic
dysfunction proportionate to increasing level of blood
pressure.
The most common presenting complaint in this study
was shortness of breath whilst the most common presenting
sign was pulmonary oedema. A previous study in Ghana
[22] found fluid overload as the most common clinical
presentation of heart failure patients. Uncontrolled
hypertension leads to neuro-hormonal activation which
eventually results in concentric left ventricular hypertrophy.
In the absence of appropriate therapy, concentric left
ventricular hypertrophy may lead to impaired left
ventricular relaxation and pulmonary oedema. ECG LVH
and echocardiographic LVH were seen in 75.56 % and
83.33 % of the patients in this study respectively. This
finding shows that the majority of the patients had already
developed left ventricular remodeling.
The prevalence of heart failure with preserve ejection
fraction (HFPEF) was high (62.22 %) in this study. Only
37.78 % of the patients presented with left ventricular
systolic dysfunction with or without a diastolic dysfunction.
This finding is different from an earlier report from Nigeria
[31]. It was found in Zaria, Nigeria that 87.4 % of
hypertensive heart failure patients presented with left
ventricular systolic dysfunction with or without a diastolic
dysfunction, whilst 12.6 % of the patients presented with
isolated left ventricular diastolic dysfunction (HFPEF) [31].
As it has been explained earlier, left ventricular diastolic
dysfunction is a major problem in patients with
hypertensive heart disease. When left ventricular
hypertrophy is detected early, appropriate therapy can lead
to reverse remodeling and prevent the occurrence of left
ventricular diastolic dysfunction.
6. Conclusion
The most common clinical presentation of patients seen
at KATH, Kumasi, with hypertensive heart failure were
shortness of breath, easy fatiguability, pulmonary oedema
and displaced apex beat. The prevalence of heart failure
with preserved ejection fraction (HFPEF) among the
patients was high.
Conflict of Interest
The authors confirm that this article content has no
conflict of interest.
Acknowledgement
The authors would like to express their sincere gratitude
to the staff at the department of medicine, Komfo Anokye
Teaching Hospital, Kumasi, Ghana for their support.
Without their co-operation this study would not have been
done.
References
[1]
Opie LH, Seedat YK. Hypertension in sub-Saharan African
populations. Circulation. 2005;112:35623568.
[2]
Kengne AP, Awah PK, Fezeu L, Mbanya JC. The burden of
high blood pressure and related risk factors in urban subSaharan Africa. Evidence from Douala in Cameroon. Afr
Health Sci. 2007;7:3844.
[3]
Plange-Rhule J, Philips R, Acheampong JW, Sagar-Malik
AK, Cappuccio FP, Eastwood JB. Hypertension and renal
failure in Kumasi, Ghana. J Hum Hyp 1999; 13: 37-40.
[4]
Falase AO, Ayeni O, Sekoni GA, Odia OJ. Heart failure in
Nigerian hypertensives. Afr J Med Sci 1983; 12: 7-15.
[5]
Van der Sande MA. Cardiovascular disease in sub-Saharan
Africa: a disaster waiting to happen. Neth J Med.
2003;61:3236.)
[6]
Owusu IK. Causes Of Heart Failure As Seen In Kumasi,
Ghana: The Internet Journal of Third World Medicine. 2007;
Volume 5, Number 1.
[7]
Amoah AG, Kallen C. Aetiology of heart failure as seen
from a National Cardiac Referral Centre in Africa.
Cardiology 2000; 93 (1-2): 11-18.
[8]
Owusu IK, Boakye YA (2013) Prevalence and Aetiology of
Heart Failure in Patients Seen at a Teaching Hospital in
Ghana. J Cardiovasc Dis Diagn 1: 131. doi:10.4172/23299517.1000131
[9]
Mendez GF, Cowie MR (2001) The epidemiological
features of heart failure in developing countries: a review of
the literature. Int J Cardiol 80: 213-219.
[10] Damasceno A, Cotter G, Dzudie A, Sliwa K, Mayosi BM.
Heart failure in sub-saharan Africa: time for action. J Am
Coll Cardiol 2007; 50(17): 688-93.
Open Science Journal of Clinical Medicine 2014, 2(1): 39-43
[11] Toure LA, Salissou O, Chapko MK. Hospitalisations in
Niger (West Africa) forcomplications from arterial
hypertension. Am J Hypertens 1992, 5: 322-324.
[12] Cooper RS, Amoah AG, Mensah GA. High blood pressure:
the foundationfor epidemic cardiovascular disease in
African populations. Ethn Dis. 2003; 13 (2 Suppl 2): S48S52.
[13] Isezuo AS, Omotoso ABO, Gaye A, et al. One year survival
among sub-Saharan Africans with hypertensive heart failure.
Tropical Cardiology 2000; 26/no 103: 57-60.
[14] Kizer, JR, Arnett, DK, Bella, JN, et al. Differences in left
ventricular structure between black and white hypertensive
adults: the Hypertension Genetic Epidemiology Network
study. Hypertension 2004; 43:1182.
[15] Van Hoeven, KH, Factor, SM. A comparison of the
pathologic spectrum of hypertensive, diabetic and
hypertensive-diabetic heart disease. Circulation 1990;
82:848.
[16] Dzau, VJ. Tissue renin-angiotensin system in myocardial
hypertrophy and failure. Arch Intern Med 1993; 153:937.
[17] Araoye MA, Olowoyeye O. The clinical spectrum of
hypertensive heart failure: a point score system for solving
an old problem. East Afr. Med J. 1984; 61:306-315.
[18] McKee PA, Castelli WP, McNamara PM, Kannel WB (1971)
The natural history of congestive heart failure: the
Framingham study. N Engl J Med 285: 1441-1446.
[19] Chobanian AV, Bakris GL, Black HR, Cushman WC, Green
LA, et al. (2003) The seventh report of the Joint National
Committee on Prevention, Detection, Evaluation, and
Treatment of High Blood Pressure: the JNC 7 report. JAMA
289: 2560-2571.
[20] Lemogoum D, Seedat YK, Mabadeje AF, Mendis S, Bovet P,
et al. (2003) Recommendations for prevention, diagnosis
and management of hypertension and cardiovascular risk
factors in sub-Saharan Africa. J Hypertens 21: 1993-2000.
[21] Scott R. C. The electrocardiographic diagnosis of left
43
ventricular hypertrophy. Am Heart J. 1960; 59:155.
[22] Owusu IK. Treatment Of Heart Failure In A Teaching
Hospital In Ghana, West Africa. The Internet Journal of
Third World Medicine. 2007 Volume 4 Number 2.
[23] Isezuo AS, Omotoso AB, Araoye MA, Carr J, Corrah T.
Determinants of prognosis among black Africans with
hypertensive heart failure. Afr J Med Sci. 2003 Jun; 32 (2):
143-149.
[24] Oyoo GO, Ogola EN. Clinical and socio demographic
aspects of congestive heart failure patients at Kenyatta
National Hospital, Nairobi. East Afr Med J. 1999 Jan; 76 (1):
23-27.
[25] Owusu IK. Electrocardiographic Left Ventricular
Hypertrophy In Patients Seen With Hypertensive Heart
Failure . The Internet Journal of Third World Medicine.
2007 Volume 6 Number 1.
[26] Task Force report. Guidelines for the diagnosis and
treatment of chronic heart failure, European Society of
Cardiology. Eur Heart J (2001) 22, 1527-1560.
[27] Ho KKL, Pinsky JL, Kannel WB, Lery D. The
epidemiology of heart failure: The Framingham study. J Am
Coll Cardiol 1993; 22 (Supplement A): 6A - 13A.
[28] Kolo PM, Jibril YB, Sanya EO, et al. Hypertension-Related
Admissions and Outcome in a Tertiary Hospital in Northern
Nigeria. International Journal or Hypertension volume 2012.
[29] Psaty BM, Furberg CD, Kuller LH, et al. Association
between blood pressure level and the risk of myocardial
infarction, stroke and total mortality: The Cardiovascular
Health Study. Arch Intern Med 2001; 161:1183-1192.
[30] Ike SO, Onwubere BJ. The relationship between diastolic
dysfunction and the level of blood pressure in Blacks. Ethn
Dis. 2003; 13(4): 463 - 469.
[31] Oyati IA, Danbauchi SS, Alhassan MA, Isa MS. Diastolic
Dysfunction in Persons with Hypertensive Heart Failure.
Journal of the National Medical Association, 2004; Vol. 96,
No. 7.
Você também pode gostar
- tmp3CAB TMPDocumento16 páginastmp3CAB TMPFrontiersAinda não há avaliações
- tmp6F0E TMPDocumento12 páginastmp6F0E TMPFrontiersAinda não há avaliações
- tmpEFCC TMPDocumento6 páginastmpEFCC TMPFrontiersAinda não há avaliações
- tmpCE8C TMPDocumento19 páginastmpCE8C TMPFrontiersAinda não há avaliações
- tmp80F6 TMPDocumento24 páginastmp80F6 TMPFrontiersAinda não há avaliações
- tmpF178 TMPDocumento15 páginastmpF178 TMPFrontiersAinda não há avaliações
- Tmp1a96 TMPDocumento80 páginasTmp1a96 TMPFrontiersAinda não há avaliações
- tmpE3C0 TMPDocumento17 páginastmpE3C0 TMPFrontiersAinda não há avaliações
- Tmpa077 TMPDocumento15 páginasTmpa077 TMPFrontiersAinda não há avaliações
- tmpFFE0 TMPDocumento6 páginastmpFFE0 TMPFrontiersAinda não há avaliações
- tmpE7E9 TMPDocumento14 páginastmpE7E9 TMPFrontiersAinda não há avaliações
- tmpF407 TMPDocumento17 páginastmpF407 TMPFrontiersAinda não há avaliações
- tmpF3B5 TMPDocumento15 páginastmpF3B5 TMPFrontiersAinda não há avaliações
- tmp72FE TMPDocumento8 páginastmp72FE TMPFrontiersAinda não há avaliações
- tmp6382 TMPDocumento8 páginastmp6382 TMPFrontiersAinda não há avaliações
- tmpD1FE TMPDocumento6 páginastmpD1FE TMPFrontiersAinda não há avaliações
- tmpC0A TMPDocumento9 páginastmpC0A TMPFrontiersAinda não há avaliações
- tmp4B57 TMPDocumento9 páginastmp4B57 TMPFrontiersAinda não há avaliações
- tmp60EF TMPDocumento20 páginastmp60EF TMPFrontiersAinda não há avaliações
- tmp998 TMPDocumento9 páginastmp998 TMPFrontiersAinda não há avaliações
- tmp8B94 TMPDocumento9 páginastmp8B94 TMPFrontiersAinda não há avaliações
- tmp37B8 TMPDocumento9 páginastmp37B8 TMPFrontiersAinda não há avaliações
- Tmp75a7 TMPDocumento8 páginasTmp75a7 TMPFrontiersAinda não há avaliações
- tmpA0D TMPDocumento9 páginastmpA0D TMPFrontiersAinda não há avaliações
- tmp9D75 TMPDocumento9 páginastmp9D75 TMPFrontiersAinda não há avaliações
- tmpB1BE TMPDocumento9 páginastmpB1BE TMPFrontiersAinda não há avaliações
- tmp2F3F TMPDocumento10 páginastmp2F3F TMPFrontiersAinda não há avaliações
- tmp27C1 TMPDocumento5 páginastmp27C1 TMPFrontiersAinda não há avaliações
- tmpC30A TMPDocumento10 páginastmpC30A TMPFrontiersAinda não há avaliações
- tmp3656 TMPDocumento14 páginastmp3656 TMPFrontiersAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (120)
- Circulatory System NotesDocumento31 páginasCirculatory System NotesJMHenry0% (1)
- Development of Heart & Vasculature - Part 1 - F2023 - DR D CostaDocumento25 páginasDevelopment of Heart & Vasculature - Part 1 - F2023 - DR D CostaJose PerezAinda não há avaliações
- Modeling and Identification of Human Heart SystemDocumento7 páginasModeling and Identification of Human Heart Systemمحمد العراقيAinda não há avaliações
- Cardiac Physiology: David Rendra Mahardika SMF Anestesiologi Dan Terapi Intensif FK UNUD/RSUP Sanglah DenpasarDocumento29 páginasCardiac Physiology: David Rendra Mahardika SMF Anestesiologi Dan Terapi Intensif FK UNUD/RSUP Sanglah DenpasarEka AriasyahAinda não há avaliações
- 2018 - Cardiac Cycle - Educational Game PDFDocumento9 páginas2018 - Cardiac Cycle - Educational Game PDFashraf alaqilyAinda não há avaliações
- Degenerative Disorders: by Dr. Madiha Ehsan UlhaqDocumento31 páginasDegenerative Disorders: by Dr. Madiha Ehsan UlhaqMohad HaiderAinda não há avaliações
- CCF Lesson Plan1Documento33 páginasCCF Lesson Plan1Topeshwar TpkAinda não há avaliações
- Anatomical Dissection GuideDocumento4 páginasAnatomical Dissection GuideLidy HigueraAinda não há avaliações
- Anatomy & PhysiologyDocumento11 páginasAnatomy & PhysiologyArah Lyn ApiagAinda não há avaliações
- TAPSE AgainDocumento8 páginasTAPSE Againomotola ajayiAinda não há avaliações
- The Heart LA WorksheetDocumento4 páginasThe Heart LA Worksheeteas grade04Ainda não há avaliações
- Circulatory System: Normel C. Adarve, RMT, MPH, IM (ASCP)Documento51 páginasCirculatory System: Normel C. Adarve, RMT, MPH, IM (ASCP)Aila AganaAinda não há avaliações
- Ayurveda Q&A - Detoxification Therapy Cures Fungal Infection - Sify HealthDocumento12 páginasAyurveda Q&A - Detoxification Therapy Cures Fungal Infection - Sify Healthsanti_1976Ainda não há avaliações
- ArrhythmiaDocumento8 páginasArrhythmiaPrecious Grace CabahugAinda não há avaliações
- DORVDocumento5 páginasDORVkelly christyAinda não há avaliações
- Clinical Experience With Affinity Pixie™ Oxygenation System in Paediatric and Infant PatientsDocumento5 páginasClinical Experience With Affinity Pixie™ Oxygenation System in Paediatric and Infant Patientsفرید رضاییAinda não há avaliações
- Heartbeat Sequencing Colour by NumbersDocumento5 páginasHeartbeat Sequencing Colour by NumbersKavs KitchensAinda não há avaliações
- 1.anatomi KVDocumento40 páginas1.anatomi KVDiiah AyuAinda não há avaliações
- BSFCR Cardio Case Group 1Documento23 páginasBSFCR Cardio Case Group 1Qurrataini IbanezAinda não há avaliações
- Anatomy Lecture Notes Unit 7 Circulatory System - The Blood Vessels-1Documento10 páginasAnatomy Lecture Notes Unit 7 Circulatory System - The Blood Vessels-1hungerfighterAinda não há avaliações
- Sample Paper - Campus Recruitment Test-Zoology PDFDocumento5 páginasSample Paper - Campus Recruitment Test-Zoology PDFAbhijeet ParkhiAinda não há avaliações
- Pocket Reference For ECGs Made Easy 5th EditionDocumento133 páginasPocket Reference For ECGs Made Easy 5th EditionSylvia Loong100% (2)
- Modulo 1 - Estructura y FuncionDocumento27 páginasModulo 1 - Estructura y FuncionYahn Carlos M MAinda não há avaliações
- Mechanical Complication of Myocardial InfactionDocumento9 páginasMechanical Complication of Myocardial InfactionDaniela VillarAinda não há avaliações
- Updated Physiology and Pathophysiology of CSF Circulation - The Pulsatile Vector TheoryDocumento18 páginasUpdated Physiology and Pathophysiology of CSF Circulation - The Pulsatile Vector TheorysavitageraAinda não há avaliações
- Bio 202 - Exam 1 (Part 2)Documento6 páginasBio 202 - Exam 1 (Part 2)GretchenAinda não há avaliações
- Anatomy NstemiDocumento3 páginasAnatomy NstemiSheana Tmpl100% (1)
- Identifying Newborns With Critical Congenital Heart DiseaseDocumento32 páginasIdentifying Newborns With Critical Congenital Heart DiseaseHardian RakhmawardanaAinda não há avaliações
- Martini The HeartDocumento64 páginasMartini The HeartEvan PermanaAinda não há avaliações
- Circulatory SystemDocumento22 páginasCirculatory SystemAliAshalAinda não há avaliações