Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Examination Obstetrics Gynaecology - 3E (PDF) (UnitedVRG) PDFDocumento325 páginasExamination Obstetrics Gynaecology - 3E (PDF) (UnitedVRG) PDFBernardo Fernandez SalazarAinda não há avaliações
- 2.1.1 Reproductive Systems Teacher Answer SheetDocumento3 páginas2.1.1 Reproductive Systems Teacher Answer SheetFerdi Hasan100% (1)
- Uterus TransplantationDocumento28 páginasUterus TransplantationJayaprakash SivamaniAinda não há avaliações
- NSVD Case StudyDocumento11 páginasNSVD Case StudyMichael UrrutiaAinda não há avaliações
- The Human Reproductive SytemDocumento23 páginasThe Human Reproductive SytemAbegail Bugayong ViceraAinda não há avaliações
- Chapter 2 - Tatiana BennettDocumento7 páginasChapter 2 - Tatiana BennettEunice CortésAinda não há avaliações
- MRCOG Part 2 Exam March 2016Documento30 páginasMRCOG Part 2 Exam March 2016Hasan Dahamsheh86% (7)
- Obstetrics & GynecologyDocumento10 páginasObstetrics & GynecologyRaul DoctoAinda não há avaliações
- Final SLE4 ThedDocumento95 páginasFinal SLE4 Thednavi_khiAinda não há avaliações
- Empanelled Surgeons 2021-22Documento30 páginasEmpanelled Surgeons 2021-22RAM KALYANAinda não há avaliações
- Geno DermaDocumento24 páginasGeno DermaNicky Adi SaputraAinda não há avaliações
- Geno DermaDocumento24 páginasGeno DermaNicky Adi SaputraAinda não há avaliações
- Gang KeratinDocumento10 páginasGang KeratinNicky Adi SaputraAinda não há avaliações
- Progestogen For Treating Threatened Miscarriage (Review) : Wahabi HA, Abed Althagafi NF, Elawad MDocumento16 páginasProgestogen For Treating Threatened Miscarriage (Review) : Wahabi HA, Abed Althagafi NF, Elawad MNicky Adi SaputraAinda não há avaliações
- DHF Menurut WHO 2011Documento212 páginasDHF Menurut WHO 2011Jamal SutrisnaAinda não há avaliações
- Depression and Risk of Stroke in Midaged Women: A Prospective Longitudinal StudyDocumento6 páginasDepression and Risk of Stroke in Midaged Women: A Prospective Longitudinal StudyNicky Adi SaputraAinda não há avaliações
- HuyuiyhhioDocumento160 páginasHuyuiyhhioNicky Adi SaputraAinda não há avaliações
- START Triage MnemonicDocumento12 páginasSTART Triage Mnemonicwawa3385Ainda não há avaliações
- PalsDocumento12 páginasPalsGhadeer EbraheemAinda não há avaliações
- PalsDocumento12 páginasPalsGhadeer EbraheemAinda não há avaliações
- Posttraumatic Stress Disorder and Adherence To Medications in Survivors of Strokes and Transient Ischemic AttacksDocumento7 páginasPosttraumatic Stress Disorder and Adherence To Medications in Survivors of Strokes and Transient Ischemic AttacksNicky Adi SaputraAinda não há avaliações
- Jurnal Lani 2Documento4 páginasJurnal Lani 2Nicky Adi SaputraAinda não há avaliações
- Depression and Risk of Stroke in Midaged Women: A Prospective Longitudinal StudyDocumento6 páginasDepression and Risk of Stroke in Midaged Women: A Prospective Longitudinal StudyNicky Adi SaputraAinda não há avaliações
- 15 Chapter 41 CoronavirusesDocumento11 páginas15 Chapter 41 CoronavirusesNicky Adi SaputraAinda não há avaliações
- Peer Group Education Effective Drug Abuse PreventionDocumento2 páginasPeer Group Education Effective Drug Abuse Preventionrezky_jbtAinda não há avaliações
- Stroke 2012 El Husseini 1609 16Documento13 páginasStroke 2012 El Husseini 1609 16Nicky Adi SaputraAinda não há avaliações
- ?DD R/ T 1 Qussg: Alamat Iido, Go 'Documento1 página?DD R/ T 1 Qussg: Alamat Iido, Go 'Nicky Adi SaputraAinda não há avaliações
- Field Statement8Documento24 páginasField Statement8Nicky Adi Saputra100% (1)
- Hematology Quiz AnswersDocumento8 páginasHematology Quiz AnswersNicky Adi SaputraAinda não há avaliações
- Hasil Analisis ALLLDocumento7 páginasHasil Analisis ALLLrezky_jbtAinda não há avaliações
- Arthropod-Born VirusesDocumento3 páginasArthropod-Born VirusesNicky Adi SaputraAinda não há avaliações
- Abs TrakDocumento17 páginasAbs TrakNicky Adi SaputraAinda não há avaliações
- Tugas Teguh 1Documento10 páginasTugas Teguh 1Nicky Adi SaputraAinda não há avaliações
- Data PenelitianDocumento2 páginasData PenelitianNicky Adi SaputraAinda não há avaliações
- Field Statement8Documento24 páginasField Statement8Nicky Adi Saputra100% (1)
- Prevention of PreeclampsiaDocumento9 páginasPrevention of PreeclampsiaSabujDasAinda não há avaliações
- Amoxicillin Clavulanate For Infections in Infants.5Documento10 páginasAmoxicillin Clavulanate For Infections in Infants.5Nicky Adi SaputraAinda não há avaliações
- LP Tumor Mamae OkDocumento13 páginasLP Tumor Mamae OkDiban namiAinda não há avaliações
- The - 2020 - Genitourinary Syndrome - of MenopausDocumento17 páginasThe - 2020 - Genitourinary Syndrome - of MenopausC T AAinda não há avaliações
- DysmenorrheaDocumento35 páginasDysmenorrheaIan Kenneth CudiamatAinda não há avaliações
- Tips For A Healthy Vagina.: Every Person Is Different. Learn What Is Normal For YouDocumento2 páginasTips For A Healthy Vagina.: Every Person Is Different. Learn What Is Normal For Youjason manalotoAinda não há avaliações
- Checklist Female GenitaliaDocumento2 páginasChecklist Female GenitaliaJessoliver GalvezAinda não há avaliações
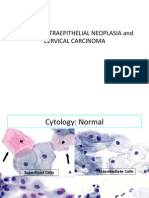
- 04 CIN and Cervical Cancer UNEDITEDDocumento120 páginas04 CIN and Cervical Cancer UNEDITEDRalph JuicoAinda não há avaliações
- Angeles y Demonios (Benni Hinn)Documento147 páginasAngeles y Demonios (Benni Hinn)Jonatan CabreraAinda não há avaliações
- Menopause Pharmacy PDFDocumento9 páginasMenopause Pharmacy PDFPhillip Doran Staver Jr.Ainda não há avaliações
- Prolonged LaborDocumento32 páginasProlonged Labormaezu50% (2)
- GYNAC Contact Update and Qualification TrackerDocumento4 páginasGYNAC Contact Update and Qualification TrackerAvinash ShrivastavaAinda não há avaliações
- Predictors For Response To Letrozole As An Ovulation Induction in Anovulatory Infertile Polycystic Ovarian Syndrome WomenDocumento23 páginasPredictors For Response To Letrozole As An Ovulation Induction in Anovulatory Infertile Polycystic Ovarian Syndrome WomenAndre OpaAinda não há avaliações
- Cervical Cancer Screening GuideDocumento45 páginasCervical Cancer Screening GuidePopa ElenaAinda não há avaliações
- History Obs & Gynae PDFDocumento4 páginasHistory Obs & Gynae PDFMaya MohamedAinda não há avaliações
- Carti Electronice OfflineDocumento33 páginasCarti Electronice OfflineCorinaAinda não há avaliações
- Labial Adhesions: Publication DetailsDocumento7 páginasLabial Adhesions: Publication DetailsSweatenia MahagoniAinda não há avaliações
- 1 SMDocumento10 páginas1 SMVina GraciaAinda não há avaliações
- New Estrogen and ProgesteroneDocumento39 páginasNew Estrogen and ProgesteroneWegrimel AriegaraAinda não há avaliações
- Shaukat Khanum Memorial Cancer Hospital Pathology ReportDocumento2 páginasShaukat Khanum Memorial Cancer Hospital Pathology ReportYaseen JamilAinda não há avaliações
- Maternal Quiz 1Documento59 páginasMaternal Quiz 1Teresa DumalagAinda não há avaliações
- MCN Nursing 1Documento107 páginasMCN Nursing 1Fau Fau DheoboAinda não há avaliações